Download
1 / 97
970 likes | 1.12k Views
Explore detailed anatomy, examinations, and common diseases like cancers in the oral cavity. Learn about diagnosis, risk factors, and patient evaluation. An essential resource for medical practitioners and students.

E N D
DISEASES OF THE ORAL CAVITY Yrd.Doç.Dr. Rasim YILMAZER Otolaryngology Department Yeditepe University School of Medicine
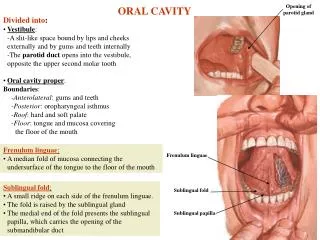
ANATOMY OF THE ORAL CAVITY • anterior : vermillion border of the lips • posterior: oropharynx • oropharyngeal isthmus : (superior) junction of the hard and soft plates . (lateral) anterior tonsillar pillars (inferior) the line of the circumvallate papillae
ANATOMY OF THE ORAL CAVITY 1- Lips 2- Anterior portion of the tongue 3- Buccal mucosa 4- Upper and lower alveolar ridges 5- Retromolar trigone 6- Floor of the mouth 7- Hard palate
Exam: Lips-palpation • Color, consistency • Area for blocked minor salivary glands • Lesions, ulcers
CANCERS OF THE LIP • 88-98% lower lip • 2-7% upper lip • 0,09-6,1% oral commisure • Male and older than 60 years old • SCC • Basal cell ca, melanoma, minör salivary gland tm.
Sensory innervation of the tongue • 1 – chorda tympani and lingual nerve • 2 – glossopharyngeal nerve • 3 – vagal nerve
Motor innervation of the tongue • Extrinsic muscles of the tongue are innervated by cranial nerve XII -Genioglossus -Hyoglossus -Styloglossus -Palatoglossus • Intrinsic muscles of the tongue are also innervated by cranial nerve XII -Superior longutudinal -Inferior longutudinal -Vertical -Transverse
Exam: Tongue • You may observe lingual varicosities
Exam: Tongue • You may observe geographic tongue (erythema migrans)
Exam: Tongue • You may observe drug reaction
Exam: Tongue • Observe signs of nutritional deficiencies
Exam: Tongue • You may observe cancer
CANCERS OF TONGUE • Lateral border • Ocult met. 30% • No supraomohyoid dissection • T1- T2 surgery or RT • T3- T4 surgery+RT • Stage, nodal metastases, lenfovasculer, perineural invasion and thickness of tumor are important prognostic factors.
Examination: Buccal Mucosa • Linea alba • Stenson’s duct
Examination: Buccal Mucosa • Lesions – white, red • Lichen Planus, Leukedema
CANCER OF THE BUCCAL MUCOSA • Advanced stage • Tm pterigoid muscles, maxilla, mandible, skin • clinic N(+)RND or MRND + cheek resection • There is no natural barrier • T1 surgery or RT • T2 surgery or RT • T3 and T4 surgery+ RT
CANCERS OF THE GINGIVA AND ALVEOLAR RIDGE • 80 % lower gingiva and 1/3 posterior region. • Incidance of mandibular invasion rate is high • upper gingiva invasion of maksillary sinus • Pull out the tooth invasion of bone marrow • uncommon • Lower jaw ( posterior 1/3 dental arch) • Marginal mandibular resection • Stage 1-2 , surgery • Stage 3-4 ,surgery+ (+) neck MRND (-) Neck Rtx
Exam: Retromolar trigone Edentulous
RETROMOLAR TRİGONE CA • Uncommon • Invasion of mandible • Late diagnose , advanced stage, cervical metastases are bad prognostic factors • T1 T2 surgery or RT • T3 T4 surgery + RT
Exam: Floor of mouth • Visualize, palpate - bimanually • Wharton’s duct • Must dry to observe • Does “lesion” wipe off? • Where are the two most likely areas for oral cancer? • lateral border of the tongue • Floor of mouth
Exam: Floor of mouth • Squamous Cell Carcinoma
FLOOR OF THE MOUTH CA. • Incidance of mandibular invasion rate is high • Ocult met 10-30% • Primary resection of the floor of the mouth is peformed with ipsilateral or bilateral neck dissection (if the tumor is located at the midline)
Exam: Hard palate • Minor salivary glands
CANCER OF THE HARD PALATE • uncommon • SCC and Adenoid cystic ca • Misdiagnosed as maxillary sinus tm • Incidance of neck metastases is low • Elective neck treatment is unnecessary • Prostodontist
ORAL PREMALİGNANCY • Leukoplakia • Erythroplakia • Mucosal atrophy
MALIGNANT LESIONS • SQUAMOUS CELL CARCINOMA • VERRUCOUS CARCINOMA • MINOR SALIVARY GLAND TUMOURS • SARCOMATOID CARCINOMAS • MALIGNANT MELANOMA
PATIENT EVALUATION Diagnosis Neoplasms of the oral cavity Complete head and neck examination Chest x-ray and liver function tests plus additional laboratory tests dictated by patient’s medical history CT/MRI scan for extent of primary and possible cervical nodal evaluation Dental evaluation Radiotherapy evaluation Staging endoscopy and biopsy
Risk factors for oral cavity and oropharyngeal cancer include: Cigarette Alcohol Exposure to the human papilloma virus (HPV) or Epstein-Barr virus (EBV) ionizing radiation Prolonged sun exposure, especially linked to cancer in the lip area and skin cancer. Fair skin, also linked to lip cancer and skin cancer. Age. People over the age of 45 years old are at increased risk for oral cancers (though it can develop in people of any age). Poor nutrition. Irritation from poorly fitting dentures in people who use alcohol and tobacco products. Chewing betel nuts, a nut containing a mild stimulant popular in Asia. Weakened immune system. Vitamin A deficiency. A rare condition called Plummer-Vinson Syndrome, which involves iron deficiency and causes difficulty swallowing. Gender. Men are more likely to get lip cancer than women. lichen planus discoid lupus erythematosus dystrophic epidermolysis bullosa ETIOLOGY
Symptoms • Otalgia • Odynofagia • Bleeding • Dysfagia • Loss of teeth • Restriction of mouth movement • Trismus