Download
1 / 22
310 likes | 706 Views
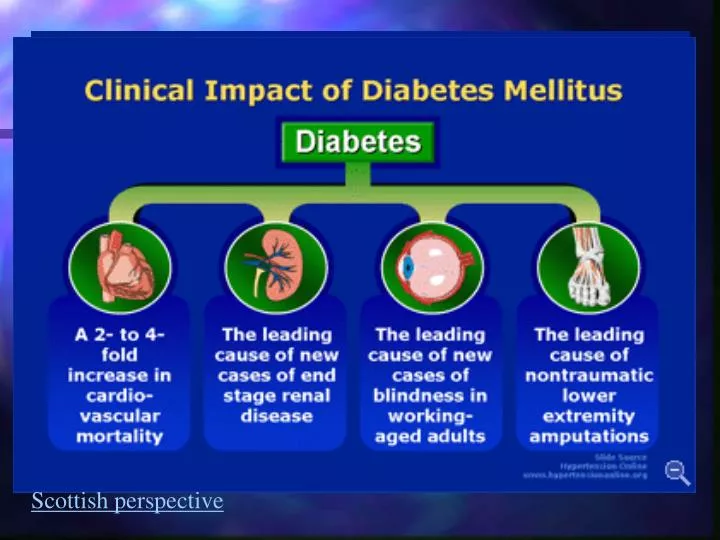
Diabetes Mellitus. Failure to control blood glucose Long term health complications Atherosclerosis Stroke Neuropathy (damaged nerves) Retinopathy, glaucoma. Scottish perspective. Control of Blood glucose. If blood glucose rises Excess is stored in muscles & liver as glycogen

E N D
Diabetes Mellitus • Failure to control blood glucose • Long term health complications • Atherosclerosis • Stroke • Neuropathy (damaged nerves) • Retinopathy, glaucoma Scottish perspective
Control of Blood glucose • If blood glucose rises • Excess is stored in muscles & liver as glycogen • If blood glucose falls • Deficit remediated by breaking glycogen down in liver and releasing into blood stream • Two hormones: • Insulin & Glucagon
Control of Blood glucose • Insulin: • Synthesised by cells of Islet of Langerhans in pancreas • Glucagon • Synthesised by cells of Islet of Langerhans in pancreas • Blood glucose level sensed in pancreas • Regulates secretion of insulin/ glucagon directly • Negative feedback system (p54)
INSULIN – target cells • Insulin acts on • Liver • Adipose tissues (fat) • Skeletal muscle cells • Insulin increases permeability of fat/ skeletal muscle cell membrane to glucose • So stimulates glucose uptake into these tissues • Liver already very permeable • Insulin stimulates glycogen formation & glucose uptake
INSULIN • Insulin acts via an insulin receptor • Diabetes occurs through two mechanisms • 1 – Loss of insulin • 2 – Loss of insulin receptors
Diabetes in Young Adults (15-30 years) Type 2 Type 1 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 Age of diagnosis
unusual genetic type of diabetes called maturity onset diabetes of the young6 different genes causing this type of diabetes.genetically defined subtype present different clinical course. one subtype responds to sulphonylureaspatients replace insulin treatment sometimes after being on insulin for over 30 years, finding the genetic cause of their diabetes has had a major impact on their treatment. Genetic Nurses in Diabetes treatment
Type 1 Diabetes – Insulin dependent • Type 1- Diabetes (5-10%) • Loss of insulin – destruction of pancreatic cells • Early onset • Weight loss, fatigue, polydypsia, polyuria, glucosuria, hyperglycaemia • Ketosis (sweet breath – due to acetone) • Treat with injections of insulin
Glucose tolerance test • A large bolus dose of glucose administered (100g glucose drink) • Blood glucose monitored • Rapid fall after peak (9-10mM) levels reached • If diabetes clearance is very slow – in urine, peak blood glucose level higher
Type 2 Diabetes – Insulin Independent • 90-95% cases of diabetes • Late onset (after 40yrs age) • 3-7% population affected • 60% SUMO wrestlers c.f. 5% Japanese population • Mainly occurs in overweight individuals
Symptoms • Insulin resistance • Normal or elevated blood insulin levels • Failure of insulin to act on target tissues • Deficiency in insulin receptors • Can lead to cell function becoming compromised due to excessive insulin production • Hyperglycaemia, polydypsia, polyuria, glucosuria
Progression • Elevated blood glucose associated with diabetes damages blood vessels and nerves • Small blood vessel damage causes blindness, kidney failure & amputation • Larger blood vessel damage can cause heart disease, high blood pressure & stroke • 75% of Type 2 patients die of cardiovascular disease
Exercise & NIDDM • Insulin sensitivity in fit individuals is greater • i.e. cells better able to uptake glucose from blood • Insulin sensitivity decreases with age • This decrease reduced by exercise • 5-7 days after exercise insulin sensitivity starts to decline • Regular, moderate, aerobic exercise is important in preventing onset of NIDDM • Diseases control in 80-90% patients achieved by reducing calorie intake/ exercise • Glasgow Research
Osteoporosis • Osteoprosis – long term progressive increase in bone porosity/ brittleness • Risk of fractures (shatter) • Loss of height • Curvature of spine • Back pain • Post menopausal women • 20-50% over 50s • 75% over 90s
Bone growth • Childhood and early adolescence bones extend • Late adolescence bones increase in density • Peak bone density in late twenties/early thirties • 1%/yr (female) decline in density thereafter • 2-3%/yr decline post menopausal • Male bone density declines 0.4%/ yr and only when over age 50 • Extra calcium/ Vitamin D in childhood & teens produce greater bone density • Margaret Thatcher – cause of osteoporosis in 2010-2020?
Elderly Early menopause Amenorrhoea Genetics Low body fat Low calcium in diet Vit. D deficiency High alcohol/ caffeine/ fizzy drinks High salt Age related reduction in bone density Oestrogen promotes calcium uptake Low oestrogen Enzymes in fat produce oestrogen from circulating precursors Body raids calcium stores in bones Poor calcium absorption Promote bone loss by using calcium stores to balance pH Calcium removed along with Na in the urine Risk Factors
Exercise & Osteoporosis – Prevention • Mechanical stress increases bone strength (density) • Astronauts have lowered bone density following zero gravity because no mechanical stress • Weight bearing or resistance exercise will benefit women in late twenties/ early thirties (swimming will not!) • Also benefits coordination reducing risk of falls
Exercise & Osteoporosis – Treatment • 45 min moderate exercise 3 times weekly increases calcium deposition in osteoporosis patients • In conjunction with HRT
Risk of Exercise in Women • Excessive exercise particularly in young women can cause osteoporosis • Reduction in body fat leads to reduction in oestrogen synthesis • Menstruation ceases • Oestrogen falls further, reducing calcium absorption • Bone loss is irreversible
Advice from Osteoporosis Soc. • It's a good idea to avoid: • Too much protein – • Excessive protein upsets acid balance. • Calcium from bones neutralises it. • Eating plenty fruit and veg should keep your body's acid balance stable. • Lots of salt – • high sodium increases calcium lost in urine. • Drinking lots of fizzy drinks – • phosphoric acid gives flavour to a lot of fizzy drinks • too much can cause the body to use calcium to balance levels. • Drinking too much caffeine – • high caffeine intake affects the balance of calcium in the body. • Milk in coffee will counteract this, limit intake to one or two cups a day. • Letting your weight drop too low – • Being underweight increases the risk of broken bones when you fall. • In younger women, severe weight loss may stop menstrual periods because hormone levels drop which can also increase your risk of breaking a bone

















