Download
1 / 31
310 likes | 509 Views
Pharmaceutical guidelines of patients with pathology of digestive organs. SYMPTOMATIC TREATMENT OF DIARRHEA. DIARRHEA. becoming more frequent (more than 3 times for the last 24 hours, for breast-feeding children more than 5-7 times) or / and dilution of feces

E N D
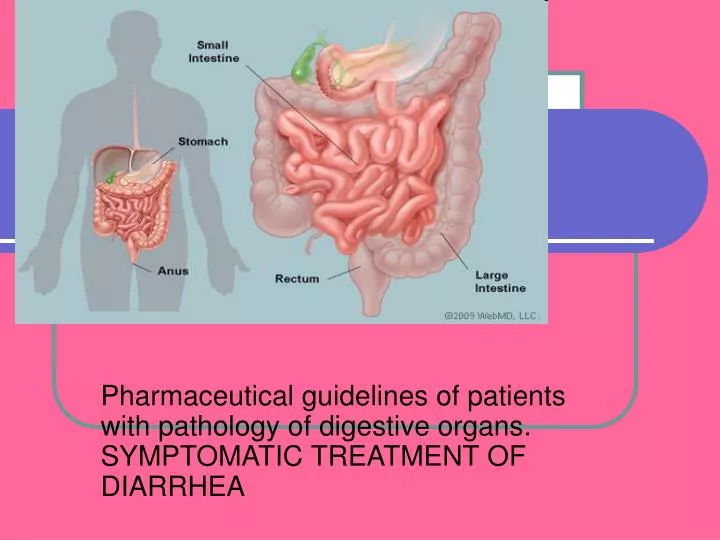
Pharmaceutical guidelines of patients with pathology of digestive organs. SYMPTOMATIC TREATMENT OF DIARRHEA
DIARRHEA • becoming more frequent (more than 3 times for the last 24 hours, for breast-feeding children more than 5-7 times) or / and dilution of feces • Diarrhea is an increase in the frequency of bowel movements or a decrease in the form of stool (greater looseness of stool). Although changes in frequency of bowel movements and looseness of stools can vary independently of each other, changes often occur in both.
Doctors classify diarrhea as "osmotic," "secretory," or "exudative" • Osmotic - something in the bowel is drawing water from the body into the bowel ("dietetic candy" or "chewing gum" diarrhea, in which a sugar substitute, such as sorbitol, is not absorbed by the body but draws water from the body into the bowel, resulting in diarrhea). • Secretory - occurs when the body is releasing water into the bowel when it's not supposed to. Many infections, drugs, and other conditions cause secretory diarrhea.
Classification (cont’d) • Exudative diarrhea refers to the presence of blood and pus in the stool. This occurs with inflammatory bowel diseases, such as Crohn's disease or ulcerative colitis, and several infections
Distinguish acute and chronic diarrhea • acute (duration less than 2-3 weeks) • chronic (duration longer than 3 weeks) It is important to distinguish between acute and chronic diarrhea because they usually have different causes, require different diagnostic tests, and require different treatment
POSSIBLE CAUSES OF DIARRHEA In patients with diseases of the gastrointestinal tract • Ulcerative colitis • As part of irritable bowel syndrome or other chronic diseases of the large intestine • Crohn's disease (ileitis terminal) • intestinal infections • Shortened guts syndrome • Endocrine dyskinesia • Chronic gastritis with decreased secretion
POSSIBLE CAUSES OF DIARRHEA In healthy individuals • Drinking milk in patients with lactase deficiency • Violation of the diet (an abrupt change of diet, water composition, the use of unripe fruit, overeating) • Scare ("bear's disease") • The use of drugs (antibiotics, antacids containing magnesium salts, potassium preparations, sulphonamides, anticoagulants, digitalis, cholestyramine, sorbitol, mannitol)
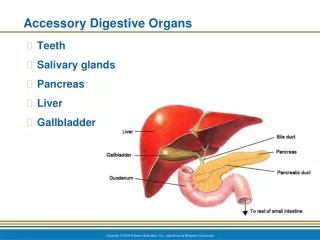
Pathogenesis • During normal digestion, food is kept liquid by the secretion of large amounts of water by the stomach, upper small intestine, pancreas, and gallbladder. • Food that is not digested reaches the lower small intestine and colon in liquid form. The lower small intestine and particularly the colon absorb the water, turning the undigested food into a more-or-less solid stool with form.
Increased amounts of water in stool can occur if the stomach and/or small intestine secretes too much fluid, the distal small intestine and colon do not absorb enough water, or the undigested, liquid food passes too quickly through the small intestine and colon for enough water to be removed. More than one of these abnormal processes may occur at the same time.
Pathogenesis (cont’d) • Some viruses, bacteria and parasitescause increased secretion of fluid, either by invading and inflaming the lining of the small intestine (inflammation stimulates the lining to secrete fluid) or by producing toxins (chemicals) that also stimulate the lining to secrete fluid but without causing inflammation. • Inflammation of the small intestine and/or colon from bacteria or from ileitis/colitis can increase the rapidity with which food passes through the intestines, reducing the time that is available for absorbing water. • Conditions of the colon such as collagenous colitis can block the ability of the colon to absorb water
Clinical symptoms • Sudden onset of bowel frequency associated with crampy abdominal pains, and a fever will point to an infective cause; • bowel frequency with loose blood-stainedstools to an inflammatory basis; • the passage of paleoffensive stools that float, often accompanied by loss ofappetite and weight loss, to steatorrhoea. • Nocturnal bowelfrequency and urgency usually point to an organic cause. • Passage of frequent small-volume stools (often formed)points to a functional cause
Threatening symptoms of diarrhea • 1. The presence of blood in the stool • 2. Feces in the form of "rice broth" • 3. Increased body temperature • 4. Nausea and vomiting • 5. Diarrhea accompanied by severe abdominal pain • 6. Diarrhea occurs in several family members • 7. Diarrhea lasts for a few weeks • 8. Diarrhea is accompanied by loss of consciousness • 9. Diarrhea accompanied by severe thirst, dry mouth, dry skin • 10. Diarrhea is accompanied by a small amount of urine • 11. Diarrhea in pregnancy
Signs of dehydration: • Dark urine • Small amount of urine • Rapid heart rate • Headaches • Dry skin • Irritability • Confusion
Signs of dehydration in young children : • Dry mouth and tongue • Sunken eyes or cheeks • No or decreased tear production • Decreased number of wet diapers • Irritability or listlessness • Skin that stays pinched instead of flattening out after being pinched
Acute diarrhea • Diarrhea of sudden onset is very common, often short-livedand requires no investigation or treatment. This type of diarrheais seen after dietary indiscretions, but diarrhea dueto viral agents also lasts 24–48 hours • Travellers’ diarrhea, which affects people travelling outsidetheir own countries, particularly to developing countries,usually lasts 2–5 days; • Clinicalfeatures associated with the acute diarrheas include fever,abdominal pain and vomiting. If the diarrhea is particularlysevere, dehydration can be a problem; • The very young andvery old are at special risk from this. • Investigations are necessaryif the diarrhea has lasted more than 1 week. Stools(up to three) should be sent immediately to the laboratory forculture and examination for ova, cysts and parasites. • If thediagnosis has still not been made, a sigmoidoscopy andrectal biopsy should be performed and imaging should beconsidered.
Acute diarrhea (cont’d) • Oral fluid and electrolyte replacement is often necessary.Special oral rehydration solutions (e.g. sodium chloride andglucose powder) are available for use in severe episodes ofdiarrhea, particularly in infants. • Antidiarrheal drugs arethought to impair the clearance of any pathogen from thebowel but may be necessary for short-term relief (e.g. Codeinephosphate 30 mg four times daily, or loperamide 2 mg threetimes daily). Antibiotics are sometimes given depending on the organism.
Chronic diarrhea • Always needs investigation. All patients should have asigmoidoscopy and rectal biopsy. • whether the large or the small bowel isinvestigated first will depend on the clinical story of, forexample, bloody diarrhoea or steatorrhoea. • When difficulties exist in distinguishing between functionaland organic causes of diarrhoea, hospital admissionfor a formal 72-hour assessment of stool weights is helpfuland will also assist in the diagnosis of factitious causes ofdiarrhoea.
Antibiotic-associated diarrhea(pseudomembranous colitis) • Pseudomembranous colitis may develop following the use ofany antibiotic. • Diarrhoea occurs in the first few days aftertaking the antibiotic or even up to 6 weeks after stopping thedrug. • The causative agent is Clostridium difficile. It is a Gram-positive, anaerobic, spore-forming bacillus and is found as part of the normal bowel flora in 3–5% of the population and even more commonly (up to 20%) in hospitalized people.
Antibiotic-associated diarrhea(pseudomembranous colitis) (cont’d)Pathogenesis • C. difficile produces two toxins: toxin A is anenterotoxin while toxin B is cytotoxic and causes bloodydiarrhoea. • It causes illness either after other bowel commensalshave been eliminated by antibiotic therapy or in debilitatedpatients who have not been on antibiotics. • Almost allantibiotics have been implicated but the present increase hasbeen attributed to the overuse of quinolones (e.g. ciprofloxacin). • Hospital-acquired infections remain high, partly due toincreased person-to-person spread and from fomites. In recent years new strains of C. difficile with greatercapacity for toxin production have been reported. There havebeen a number of hospital outbreaks with a high mortality.
Clinical features • C. difficile diarrhoea can begin anythingfrom 2 days to a month after taking antibiotics. • Elderly hospitalizedpatients are most frequently affected. It is unclearas to why some carriers remain asymptomatic. • Symptomscan range from mild diarrhoea to profuse, watery, haemorrhagiccolitis, along with lower abdominal pain. • The colonicmucosa is inflamed and ulcerated and can be covered by anadherent membrane-like material (pseudomembranouscolitis). The disease is usually more severe in the elderly andcan cause intractable diarrhoea, leading to death.
Treatment • metronidazole 400 mg three times daily or • oral vancomycin 125 mg four times daily • Causative antibioticsshould be discontinued if possible.
Travellers’ diarrhea • Travellers’ diarrhea is defined as the passage of three ormore unformed stools per day in a resident of an industrializedcountry travelling in a developing nation. • Infection isusually food- or water-borne, and younger travellers aremost often affected (probably reflecting behaviour patterns). • Reported attack rates vary from country to country, butapproach 50% for a 2-week stay in many tropical countries. • The disease is usually benign and self-limiting: treatment withquinolone antibiotics may hasten recovery but is not normallynecessary. • Prophylactic antibiotic therapy may also be effectivefor short stays, but should not be used routinely.
Purgative abuse • This is most commonly seen in females who surreptitiouslytake high-dose purgatives and are often extensively investigatedfor chronic diarrhea. • The diarrhea is usually of highvolume (> 1 L daily) and patients may have a low serumpotassium. • Sigmoidoscopy may show pigmented mucosa, acondition known as melanosis coli. Histologically the rectalbiopsy shows pigment-laden macrophages in patients takingan anthraquinone purgative (e.g. senna). • Melanosis coli isalso seen in people regularly taking purgatives in normaldoses. • In advanced cases a barium enema may show a dilatedcolon and loss of haustral pattern. • Phenolphthalein laxatives can be detected by pouring analkali (e.g. sodium hydroxide) on the stools, which then turnpink; a magnesium-containing purgative will give a highfaecal magnesium content. • Anthraquinones can also bemeasured in the urine. If the diagnosis is suspected, a lockeror bed search (while the patient is out of the ward) is occasionallynecessary. Management is difficult as most patientsdeny purgative ingestion. • Purgative abuse often occurs inassociation with eating disorders and all patients needs psychiatrichelp. It is sometimes safer not to confront the patientwith their diagnosis.
Diarrhoea in patients withHIV infection • Chronic diarrhoea is a common symptom in HIV infection,but HIV’s role in the pathogenesis of diarrhoea is unclear. • Cryptosporidium is the pathogen most commonlyisolated. Isospora belli and microsporidia have alsobeen found. • The cause of the diarrhoea is often not found and treatmentis symptomatic.
Functional diarrhea • In this form of functional bowel disease, symptoms occur inthe absence of abdominal pain and commonly are: • ■ The passage of several stools in rapid successionusually first thing in the morning. No further bowelaction may occur that day or defecation only aftermeals. • ■ The first stool of the day is usually formed, the laterones mushy, looser or watery. • ■ Urgency of defecation. • ■ Anxiety, uncertainty about bowel function with restrictionof movement (e.g. travelling). • ■ Exhaustion after the ‘morning rush’.
Treatment of functional diarrhea • loperamide oftencombined with a tricyclic antidepressant prescribed at night(e.g. clomipramine 10–30 mg).
Drugs for treatment of diarrhea • Anastaltic (loperamide) • enzyme agents (creon, festal, enzymtal, enzystal, pancreatin) • drugs for oral rehydration (gastrolit, rehydron) • Antidiarrheal microbial products, probiotics (bifidumbacterin, bificol, bifiform, colibacterin, lactobacterin, hilak) • drugs of other pharmacological groups (smecta, antispasmodics)
Pharmaceutical guardianship for diarrhea • When diarrhea is a loss of fluid and electrolytes, so you need prescriptions for oral rehydration • Loperamide administered with caution to patients with impaired liver function • If you experience constipation reception anastaltic drugs must be stopped immediately • In the appointment of loperamide may appear a pain in the lower abdomen, fatigue, lethargy, headache
Pharmaceutical guardianship for diarrhea (cont’d) • On the background of antimicrobial therapy may use probiotics or drugs linex or bifiform because they contain antibiotic-resistant strains of the intestinal flora • Unacceptably to add sugar in oral rehydration solutions (increased osmolarity of the solution and as a result - increased diarrhea) • Since Smecta has adsorbent properties, and may slow or reduce absorption of simultaneously taken drugs. It is recommended to comply with the interval between smecta doses and other drugs
Pharmaceutical guardianship for diarrhea (cont’d) • Simethicone, which is part of enzimtal, pangrol, reduces flatulence • Drugs hilak & hilak forte should not take with milk and other dairy products • Concomitant use of hilak and hilak forte with antacids is unacceptable • Laktobacterin is recommended to drink milk