Download
1 / 12
130 likes | 297 Views
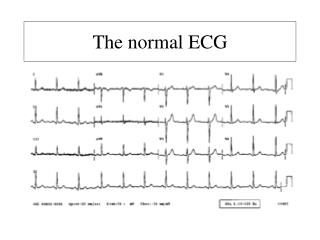
ECG Monitoring – Reference Guide. Cardiac Conduction Pathway. The ECG Tracing. Label ECG tracing w/P,Q,R, S, T and U. Label SA node, AV node, bundle of His, bundle branches and Purkinje fibers. SA node= 60-100 beats/min AV node= 40-60 beats/min Bundle of His= 40-60 beats/min

E N D
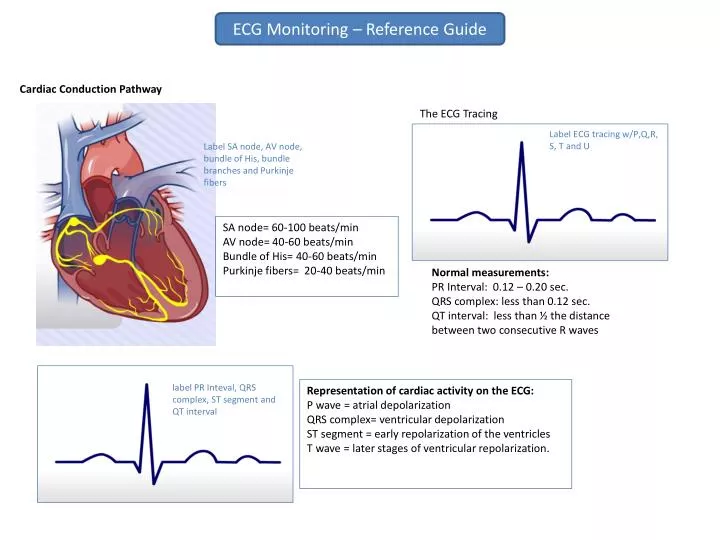
ECG Monitoring – Reference Guide Cardiac Conduction Pathway The ECG Tracing Label ECG tracing w/P,Q,R, S, T and U Label SA node, AV node, bundle of His, bundle branches and Purkinje fibers SA node= 60-100 beats/min AV node= 40-60 beats/min Bundle of His= 40-60 beats/min Purkinje fibers= 20-40 beats/min Normal measurements: PR Interval: 0.12 – 0.20 sec. QRS complex: less than 0.12 sec. QT interval: less than ½ the distance between two consecutive R waves label PR Inteval, QRS complex, ST segment and QT interval Representation of cardiac activity on the ECG: P wave = atrial depolarization QRS complex= ventricular depolarization ST segment = early repolarization of the ventricles T wave = later stages of ventricular repolarization.
ECG Monitoring – Guide to Leads View of the heart provided by each lead: 264 American Heart Association’s standard color coding for ECG leads Lead placement for 5 lead ECGs Lead placement mnemonic: White is right. Snow over trees (white over green). Smoke over fire (black over red). Chocolate (brown) is close to the heart.
ECG Monitoring – 5 Step Analysis Step 1: Assess the regularity of the rhythm Are the P waves (for atrial rhythm) or the R waves (for ventricular rhythm) consistently equidistant from each other? If there is a variation of more than 3 small boxes (0.12 seconds), the rhythm is considered irregular. The Square Counting, or Sequence, Method The square counting method can be used for regular heart rhythms. First, find an R wave that falls on a thick line. The next thick lines will be counted as follows: 300, 150, 100, 75, 60, 50, 43, 37. Stop the sequence at the next R wave. If the second R wave falls between two thick lines, use the mean of the two numbers (for example, if the R wave falls between 150 and 100, the rate would be 125) Step 2: Calculating the heart rate The Six-Second Method This method can be used to easily measure the heart rate in non-regular rhythms. To calculate the ventricular rate, simply count the number of QRS complexes in a 6 second strip and multiply by 10. To calculate the atrial rate, count the P waves instead of the QRS complexes. The Small Box Method Count the small boxes between two sequential R waves (for the ventricular rate) or two sequential P waves (for the atrial rate). Divide this number into 1500 to obtain the rate. The Large Box Method For this method, count the number of large boxes between two sequential R or P waves. Divide this number into 300 to obtain the rate.
ECG Monitoring – 5 Step Analysis 3rd Step: Assessment of the P waves The P wave represents atrial depolarization. An absent P wave indicates that the electrical impulse is being generated from somewhere other than the SA node. An inverted P wave can be seen with ectopic atrial and junctional rhythms. Peaked P waves may be seen with right atrial enlargement, usually due to pulmonary hypertension Notched P waves can be seen with left atrial enlargement, usually due to mitral stenosis. (#2b) Variable P waves are indicative of multifocal atrial rhythms (meaning multiple sites within the atrium or AV junction are acting as ectopic pacemakers). 4th Step: Assessment of the PR interval The PR interval reflects the total time it takes for the electrical impulse to travel from the SA node through the AV node into the ventricles. A shortened PR interval (> 0.12 seconds) can indicate a junctional rhythm where the impulse originates in the AV junction, or an abnormal conduction pathway. A prolonged PR interval indicates that the impulse is being delayed before entering the ventricles. This is called first degree block and can be caused by myocarditis, acute myocardial infarction, hyperkalemia, medication effects, AV septal defects and enhanced vagal tone. A variable PR interval can indicate a wandering atrial pacemaker, Wenckebach rhythm (2nd degree Mobitz Type I), 3rd degree (complete ) AV block. Additional Assessments: The T wave & the QT interval The T wave represents ventricular repolarization. It usually deflects upright in all leads except aVR and V1. Assess the T wave for abnormalities in shape or consistency and for inversion in leads where it normally is upright. T wave abnormalities may be seen with myocardial ischemia or infarction, bundle branch blocks, pulmonary embolism, electrolyte imbalances and ventricular hypertrophy, among other conditions. The QT interval represents the total time for ventricular depolarization and repolarization. Abnormalities in the QT interval can indicate risk for serious ventricular arrhythmias. Prolonged QT intervals can also be caused by medication effects, hypocalcemia, myocarditis and CNS lesions. 5th Step: Assessment of the QRS Complex The fifth step is to assess the QRS complex. The QRS complex represents ventricular depolarization. As with the PR interval, the QRS complex needs to be assessed for both duration (width) and consistency. The QRS can be classified as narrow (<0.10 sec) or wide (>0.12 sec). An abnormally wide QRS complex can indicate a delay or abnormality in conduction through the ventricle. Causes of wide QRS complexes can include bundle branch blocks, Wolff-Parkinson White syndrome, hyperkalemia, medication effects, and ventricular tachycardia, fibrillation or ectopic beats.
ECG Monitoring Arrhythmia Review Sinus Rhythms
ECG Monitoring Arrhythmia Review Sinus Rhythms (continued) Atrial Rhythms
ECG Monitoring Arrhythmia Review Atrial Rhythms (continued)
ECG Monitoring Arrhythmia Review Junctional Arrhythmias
ECG Monitoring Arrhythmia Review Ventricular Rhythms
ECG Monitoring Arrhythmia Review Ventricular Rhythms (continued)
ECG Monitoring Arrhythmia Review Atrioventricular Blocks
ECG Monitoring Arrhythmia Review Pulseless Electrical Activity Pulseless electrical activity (PEA) is not a specific arrhythmia, but occurs when an organized rhythm is seen on the ECG tracing but ventricular contraction does not occur and, therefore, the patient is pulseless. Show strip from module Pulseless electrical activity can present as various rhythms on the ECG tracing, including sinus rhythm, bradycardias and tachycardia. • Pacemakers • Pacemakers can pace either the atria or the ventricles (single chamber pacemakers) or both (dual chamber pacemakers). • In atrial pacing, a spike will be seen prior to the P wave. • In ventricular pacing, a spike will be seen before the QRS complex. • Spikes before the P wave and QRS complex will be present when the patient has a dual chamber pacemaker. Show pacemaker strips from module Pacemaker Problems Notable on the ECG Failure to pace Absence of pacemaker spikes when the patient’s heart rate is below the pacemaker rate. Failure to capture Pacemaker spikes will be seen on the ECG but they will not be followed by a P wave (in atrial pacing) or a QRS complex (in ventricular pacing). Failure to sense The pacemaker spike will be seen in an inappropriate place on the ECG (for example, after or near a QRS complex in ventricular pacing).