Download
1 / 46
460 likes | 604 Views
Dawn Moss NHS Borders Early Years Collaborative Improvement Adviser Child Protection Health Needs Assessment. Background. Why does it matter - long-term effects for child ’ s health, growth, intellectual development and mental wellbeing (NSPCC, 2010)

E N D
Dawn Moss NHS Borders Early Years Collaborative Improvement Adviser Child Protection Health Needs Assessment
Background • Why does it matter - long-term effects for child’s health, growth, intellectual development and mental wellbeing (NSPCC, 2010) • Primary drivers in EYC Workstreams 2 and 3: child’s physical, mental and emotional development • Child Protection Health Needs Assessment process established in 2013 – improvement needed to ensure that every child who needs it will have a health needs assessment
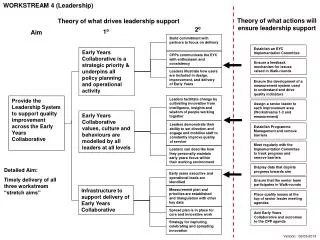
Aim Primary Drivers Secondary Drivers Specific Ideas to Test
Establish data collection process for HNA D S P A A P S D D S P A A P S D A P S D PDSA RAMP 1: Test data collection tool Cycle 5: All members of Child Protection Team to take a turn in collecting and inputting data to ensure consistency. Cycle 4: Repeat cycle 3 now that problems accessing excel spreadsheet are resolved. Cycle 3: Senior Nurse Child Protection has responsibility for collecting and inputting data onto excel spreadsheet Cycle 2: Senior Nurse Child Protection has responsibility for collecting data, additional information identified, Nurse Consultant inputs data onto excel spreadsheet Cycle 1: Child Protection Team collects data at weekly Child Protection Unit Business meeting
Improve HNA process aligned to GIRFEC D S P A A P S D D S P A A P S D A P S D PDSA RAMP 2: Test new Health Needs Assessment documentation Cycle 3:Test introduction of new form as part of HNA process with one health visitor (currently underway) Cycle 2: Test new HNA form with school nurse, no changes Cycle 1:Test new HNA form with health visitor, changes made
Staff have knowledge and resources for HNA process D S P A A P S D D S P A A P S D A P S D PDSA RAMP 3: Communication with staff Cycle 4: Test written guidance for staff (currently underway) Cycle 3: Test briefing/workshop format (currently underway) Cycle 2: Test feedback form to health visitors/school nurse when HNA request (currently underway) Cycle 1: Communication via email to paediatricians re having discussion at end of weekly Child Protection Unit Meeting for all children discussed to be considered for HNA
Reflections • Worrying about measures – I’m doing it wrong • Lots of activity but no run charts! • Not knowing what is wrong, not knowing what questions I need to ask! • Knight in shining armour.... ta-da... Brandon Bennett • Knowing your process – steps – decision points • “Moving from objective reality to belief”
Michelle Dowling South Lanarkshire Pioneer Site: Maximising income for pregnant women
Background • Telephone advice line (TAL) for pregnant women, funded from SL Tackling Poverty Programme • Lower than expected referrals from universal NHS midwifery services • Focus initially to increase referrals from community midwives to service • Initial tests post LS1 – one midwife in Hamilton; tested a number of change ideas
Phase 1 testing Aim: to increase referrals from community midwifery services to the TAL Measure(s): NO. of referrals from midwifery staff to TAL: Result: initial rise; but slows. Think again Change Ideas: midwife speaks to women routinely as part of visit; use of case studies; Are we ready to scale up? Learning from data Cycle 5: start test with another midwife in EK. Cycle 4: stop using case studies but feel change is embedded. Cycle 3: case studies used to promote the service with women. Cycle 2: information about service given to women as part of visit as well as discussion with midwife: Cycle 1 : Helen in Hamilton is recruited to test new ways of promoting service. She starts speaking to women as part of routine visits.
Run chart data Use of case studies – stopped following data protection concerns
Add a new site...Run Chart Data suggests no increase in Hamilton overall and EK little or no change.
What changes will make a difference? Secondary drivers Primary drivers Aim Focus of current tests Women allow midwifery staff to pass details to TAL for phone back Staff working with ante-natal women refer clients to service Financial advice services and information are available and accessible Midwifery staff routinely talk to women about the TAL FNP/First Stepsstaff routinely refer women to TAL or other service Financial advice services have specialist knowledge to support pregnant women Women get the information they need when they need it All pregnant women on low incomes have the opportunity to maximise their incomes during pregnancy and in the first year of their child’s life Staff member with good generic knowledge of financial issues linked to midwifery team Opportunities for other forms of income support are available and accessible Redesigned leaflets with input from potential and past service users increase women’s knowledge Women take up Healthy start vouchers and vitamins Women and their partners have access to information on training and employment schemes Pregnant women need support to be able to budget and manage their money Opportunities for training and education are available and accessible Parents have access to affordable childcare
South Lanarkshire CPP: phase 2 Aim: to increase referrals from community midwifery services to the TAL Measure(s): number of referrals from midwifery staff to TAL: Result: initial rise; volume becomes an issue Change Ideas: pass contact details to TAL who phone back the women for initial discussion. Learning from data Cycle 3: (planned):more midwives in the team use this method with women in their clinics. Cycle 2: Continue to monitor Helen’s progress and a second midwife starts using the new approach : Cycle 1 : Helen starts asking women if details can be passed to TAL. Initial results seem favourable :
Reflections • Complexity of testing across services and organisations Local Authority NHS Tackling poverty (Com & Ent) EYC FNP Midwifery services Money Matters Advice Service (SW)
Reflections (2) • You don’t know what you don’t know! • Scale - one eye on full scale when starting small. • Don’t make assumptions about new practice and scale too early • Don’t forget basic project management • Volume • Much work across EYC is to improve low volume activity – implications for scaling up
Sacha Will Aberdeen City CPP Early Years Collaborative Improvement Adviser Improving Attachment-led Practice
Background • Series of multi agency training sessions held on Attachment during 2013 • 2014 – Early Adopters identified • Preschool settings incl. private childcare sector AIM: Identify, by December 2014, an evidence based change package which can improve attachment-led practice within pre-school settings in Aberdeen.
2⁰ 1⁰ Tests of Change Improving attendance at Ante Pre-School provision (WS3) Optimise development of children’s emotional well being and resilience. Attachment Evaluate support for parents (incl. Foster Carers)Pre-birth and Beyond Provision of Antenatal Education-universal as well as targeted Optimise Family Relationships Wider Communication Strategy Promoting skin on skin/ eye contact (WS1) Improve Maternal Health and Wellbeing Enhancing Secondary Education PSHE Parent/Caregiver is attuned and responsive to children’s needs. Engagement with PEEP Aim Content of Ante-natal classes Optimise Workforce Capacity to implement attachment-led practice Development of Peer networks to reduce isolation and share knowledge & understanding Developing Dad’s Work To ensure that 90% of children experience positive and secure relationships with their caregiver by June 2015, when assessed Evaluation of Attachment Training (WS4) Engage with Private Sector Consistent/ clear assessment of attachment/emotional wellbeing Workforce Development and Training Attachment Training Access to Bumps programme Developing Community Assets Develop Assets to support positive and secure attachment (Co-production) Access to support when needed. Linking Roots of Empathy Developing Co-production methods Parental engagement with projects. Early identification of Health Plan Indicators (WS1) Early Identification of parents that need support (Inc. pre-birth) Version 2: 120913
Pre-school Setting 1 • Aim: Introduce use of assessment tool and individual support plans to improve support provided for children’s emotional wellbeing by September 2014. Learning from data Cycle 5: Test use of run chart to display progress for individual children Cycle 4:Develop individual support plans for specific children Cycle 3: Test use of Leuven Scale with three practitioners and all children. Cycle 2: Test use of Leuven Scale with two practitioners and small group of children Cycle 1:Test use of Leuven Scale of Wellbeing & Involvement with one practitioner and small group of children
Pre-school Setting 2 • Aim: Introduce use of transitions worker and transitions ‘bundle’ to improve support provided for all children during settling and transitions by October 2014. Learning from data Cycle 4: Develop ‘transitions checklist’ Cycle 3: Test use of Leuven Scale for assessing children’s wellbeing during transitions Cycle 2: Introduce use of ‘key worker’ system for children who are transitioning between rooms Cycle 1: Identify areas for improvement in our transitions process
Pre-school Setting 3 • Aim: Improve ‘dropping off’ and ‘picking up’ routines for all children by October 2014. Learning from data Cycle 2: Share information with parents to identify new ‘drop off’ process Cycle 1: Use Leuven Scale of Wellbeing & Involvement to gather baseline data regarding impact of interruptions during ‘drop off’ process
Reflections Messiness of life Making assumptions is a trap! PDSA cycles help you to pay attention to the detail Always make predictions BEFORE you start to test The value of learning from others Run Charts make life easier!
Early Years Collaborative: Learning Session 5 EYC Leith Pioneer Site:income maximisation and maternal & child nutrition Graham Mackenzie on behalf of the Leith Pioneer Site team
Income Maximisation Healthy Start: • Food and vitamin vouchers • Benefits recipients • All pregnant women under 18 years of age • Pregnant women (from 10 weeks gestation) and children under 4 years old • £3.10 per week food vouchers
Aims Improvement project: To improve uptake of Healthy Start (food and vitamin voucher scheme) to 90% of eligible participants (benefits recipients, child tax credit recipients if household income < £16,190 and pregnant women under 18 years old) in selected areas of Edinburgh (initially north east Edinburgh) by March 2015 Pioneer site: To learn lessons that can be scaled up to other areas and parts of Scotland
Population segmentation 5 women per week, 20% eligible = small enough?
One midwife Timeline 6 weeks? 8-9 weeks 10 weeks 11-13 weeks 16 weeks 25 weeks Woman’s antenatal care Woman finds out she is pregnant Calls central booking line “Booking” appointment with midife Ultrasound scan Midwife appointment Midwife appointment HS process: Before Appn form may be given at this point Appn form completed now… …if remember to bring it… …or now HS process: After Appn form completed
PDSA Ramp (for antenatal work) DATA FEEDBACK TO FRONTLINE STAFF: Compliance w PVC check D S P A A P S D D S P A A P S D A P S D Scaling up: Survey with other team identified similar areas for improvement (n=7). Working with two midwives in that team to incorporate lessons from Leith team. Preparing to spread simple messages across Lothian (Further survey completed by 61 midwives). Increased registration at antenatal booking PDSA 7. Reinforced messages with team by collecting information in survey and fed back results at team meeting (n=19). PDSA 6. Midwife shared simpler application process with colleagues at team meeting (n=19 midwives in team). PDSA 5. Identified simpler application process and tested this with same midwife: no need for ultrasound as proof of pregnancy, complete midwife section of application form at booking visit (initially n=1). (PDSA 4. Workwith Health visitor team and welfare rights advisor). PDSA 3. Time between centralised booking call and appointment was 2-4 weeks, and first 8 women were seen by 5 different midwives, so shifted to look at caseload of single midwife, with routine enquiry about eligibility for Healthy Start (n=1). PDSA 1. The health records team identified women from two postcode sectors calling the centralised booking line. They inserted a letter and Healthy Start application form into the booking pack. Health records staff sent details to midwives who met women at booking visit. Shared data with health records team that showed that some women from postcode sectors were not being identified (PDSA cycle 2).
% antenatal bookers eligible for Healthy Start in Leith (self report) (n=410; source Maternity Trak) “Shift” on run chart (6+ points above median) Universal enquiry re HS Complete form at booking appt Team meeting Focus on Trak docu-mentation Monthly data release Monthly data release Leith Survey Monkey Team meeting and survey results Median Leith Pioneer site work started 3 March
Conclusions Plan small, start smaller Deming’s Lens of Profound Knowledge • understanding variation • appreciation for a system • building knowledge • human side of change Having an existing electronic record has been really useful We still have a long way to go