Download

1 / 46
460 likes | 470 Views
This presentation explores the health costs associated with traffic-related air pollution in Austria, France, and Switzerland. It highlights the need for interdisciplinary approaches and includes topics such as air pollution concentrations, population exposure distribution, epidemiology, and costing. Uncertainties and key outcome uncertainties are also discussed.

E N D
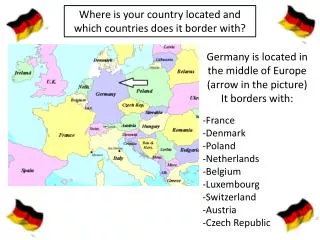
Question of the Authorities of Austria, France, & Switzerland: What are the health costs of traffic-related air pollution ? UNECE1.ppt
Requires interdisciplinary approaches Air pollution concentrations Air Hygiene Population exposure distribution GIS Exposure - Response function Epidemiology Derivation of attributable cases Epi Risk Assess. Costing Economy UNECE.ppt
Uncertainties • multiple sources of uncertainties • majority: not statistical uncertainties • conceptual and data uncertainties • gaps at interdisciplinary interface • “At least” approache • with risk function based 95% CI UNECE.ppt
Definition of Air Pollution Exposure • Availability of effect functions • Availability of exposure data • no multiple counting (correlated pollutants; same sources) • PM10 „at least“ UNECE.ppt
Selected Attributable Health outcomes Attributable Death Long-term effect Hospital admissions (cardio-resp.) Short-term effect Chronic bronchitis incidence (adults) Long-term effect Bronchitis episodes (children) Short-term effect Restricted activity days Short-term effect Asthma attacks (children & adults) Short-term effect UNECE.ppt
Impact Assessment Model # Death Exposure-response function 7.5 ug/m3 Attributable death „at least“ PM10 PM10 reference
Exposure-Response Functionfor Mortality • Weighted average of : • ACS-Study (Pope et al., 1994) • Harvard 6-City Study (Dockery et al, 1993) • 4.3 % (95% CI: 2.6-6.1%) increase per 10 g/m3 PM10 • ~ 360 (200-520) attributable death • per 10 g/m3 PM10 and 1 Mio. inhabitants UNECE.ppt
Frequency distribution of total PM10 population exposure UNECE.ppt
Air Pollution Attributable Death in Austria, France and Switzerland Attributable Death (adults ³ 30 yrs.) Total # cases: 40‘600 (24‘600-56'900) or: ~ 6% (3.6-8.4%) of total deaths Traffic related: 21’800 (13’300- 30’600) UNECE.ppt
Monetarization of attributable death in the Trinational Study source: Willingness-To-Pay estimates value: 900‘000 EUR per statistical fatality total: 36.5 Mio. EUR See: Sommer et al, in OECD Report: Ancillary Benefits and Costs of Greenhouse Gas Mitigation, New York; 2000 UNECE.ppt
Air pollution related health costs ~ 50‘000 Mio. EUR per year traffic related: ~ 27‘000 Mio EUR per year UNECE.ppt
Key Outcome Uncertainties 1) Why cohort study estimates? 2) Attributable death and life time lost 3) Are US-Studies relevant for Europe? 4) Are effects source specific? 5) Are “attributable” death “preventable” UNECE.ppt
1) Why Cohort study based Attributable Death ? OR: Why not time-series based estimates, which are 5-10 times smaller ? UNECE.ppt
Frailty and Death Frailty (susceptibility for death) Death Time Birth Age at death
Frailty and Exposure Frailty (susceptibiltiy for death) Death Time Birth Age at death Start smoking
Contribution of Air Pollution Frailty (susceptibility for death) SMOG EPISODE Death Cumulative exposure Chronic Bronchitis Time Birth Age at death
Focus of the Time-series analysis Frailty (susceptibilty for death) Death Time Birth
Time-series: counting advancement of death Death counts Pollution Time Period of exposure Time to event Period of events SHORT PERIODS SHORT PERIODS SHORT PERIODS SHORT PERIODS SHORT PERIODS UNECE.ppt
Time-series • 1) Time-series captures • short-term effects only • not all short-term effects • 2) Life time lost not known • 3) Long-term effect on life shortening not measured > > incomplete impact assessment
Focus of the Cohort Study Frailty (susceptibilty for death) Time Birth
Cohort studies • capture cumulative total effects on time to death > more complet counting of effects BUT: • no distinction of acute and long-term • only US studies • YoLL not published /QALY not assessed
Long-term and short-term cases(Künzli et al, Am J Epidemiol 2001 in press, adapted from COMEAP, 1998) All Air Pollution cases long-term effect short-term effect Mixed effects All Death
2) Number of deathversus years of life lost Both: • Life expectancy in a population • annual number of deaths depend on: age specific death rates
BUT: published are only number of deaths ! Indirect estimates of years of life lost: • life table approache • assumptions about age structure of cases
Mortality in the Trinational Study 1) Direct estimates of „attributable death“ ( > age 30; non-violent death) 2) Years of life lost: • Indirect estimates, used for costing • assumptions: • the attributable death are due to cardiopulmonary causes • same age distribution as all cardiopulmonary death • thus: typical age of an „air pollution death“ ~75-80 yrs.
Average reduction in population life expectancy For a population with a 10 g/m3 higher PM10 Sommer et al. (Trinational Study): ~0.5 yr other estimates: ~6 mo. to ~2 yrs. (Brunekreef; Pope; Leksell; Hurley; Miller; Rabl etc.)
3) We transfered the US cohort results to Europa ! • Consistency for other outcomes between US and European countries • Coherence between different outcomes UNECE.ppt
Mortality (adjusted Relative Risk) and long-term mean pollution (PM2.5)Harvard Six-City Cohort Study, Dockery et al, NEJM 1993; 329 (24):1753-9 Relative Risk mean PM2.5 UNECE.ppt
Annual mean PM10 and expiratory capacity (FVC) in the 8 SAPALDIA areas Ackermann-Liebrich et al, AJRCCM 1997; 155 (1):122-129 FVC % deviation from predicted PM10 annual mean (g / m3) UNECE.ppt
Other Evidence? Europe French PAARC suggestive abstract Dutch cohort suggestive abstract SAPALDIA ?? Needs other 10 yrs. ECRHS ?? ? USA: Abbey et al 1999 interaction with sex? Krewski et al 2000 interaction with SES? UNECE.ppt
4) Are attributable death source specific? Assumption in tri-national study: • PM10 effects are independent of PM source • -> one single effect slope UNECE.ppt
Percent Change (and 95th CI) in Daily Death per 10 g/m3PM2.5 mass an source specific elements1979-1988, Harvard Six Cities; Laden et al, Env Health Perspect 2000; 108 (10): 941-947 Motor (Pb) PM2.5 mass Coal (Se) Crustal (Si)
Percent Change (and 95th CI) in Daily Death per 10 g/m3PM2.5 mass an source specific elements1979-1988, Harvard Six Cities; Laden et al, Env Health Perspect 2000; 108 (10): 941-947 Motor (Pb) PM2.5 mass Coal (Se) Crustal (Si)
Percent Change (and 95th CI) in Daily Death per 10 g/m3PM2.5 mass an source specific elements1979-1988, Harvard Six Cities; Laden et al, Env Health Perspect 2000; 108 (10): 941-947 Motor (Pb) PM2.5 mass Coal (Se) Crustal (Si)
Percent Change (and 95th CI) in Daily Death per 10 g/m3PM2.5 mass an source specific elements1979-1988, Harvard Six Cities; Laden et al, Env Health Perspect 2000; 108 (10): 941-947 Motor (Pb) PM2.5 mass Coal (Se) Crustal (Si)
5) Are „attributable death“ also „preventable death“? UNECE.ppt
Unknown time domaines • Duration of ‘long-term’ exposure • Relevant time window of exposure • Time between exposure and effect • Time between intervention and benefit? UNECE.ppt
Time-to-Benefit (death, long-term) (Sommer et al., 1999) Attributable Costs 10 20 Time (yrs) Clean air intervention UNECE.ppt
Competing risks Removal of one long-term health risk factor will modify the importance of the remaining risks “attributable death” > “preventable death” UNECE.ppt
TSP decrease and reduction in bronchitis prevalence(Germany, 1993 versus 1995, children, age 5-14 yrs) 70 Hettstedt 60 Bitterfeld bronchitis prevalence (%) Zerbst 50 40 Year: 30 1993 30 40 50 60 70 1995 3 annual mean of TSP m g/m (Heinrich et al, AJRCCM 2000; 161:1930-36) COP6DenHaag.ppt
Acute bronchitis in children and annual mean PM10 The SCARPOL Study 25 23 Genf 21 Lugano Anières 19 Biel 17 Zürich Bern 15 Prevalence of dry cough at night (%) Langnau 13 Payerne 11 Montana 9 Rheintal 7 5 5 10 15 20 25 30 35 Annual mean PM10 mg/m3 3 m Jahresmittel PM10( g/m ) C. Braun-Fahrländer; AJRCCM 1997 UNECE.ppt
Conclusion • Air pollution accounts for 4-8% of death • “Attributable death” from cohorts: adequate approache • BUT: gaps in evidence and uncertainties: • Best effect estimate? • Years of life time lost? • European long-term studies? • Source attribution ? • How many are “preventable death”? When? UNECE.ppt
Thanks Nino.Kuenzli@unibas.ch Institute of Social and Preventive Medicine University Basel
Susceptibility and Time-to-event Probability of event • High susceptibility • Early response • Low susceptibility • Late response Time Exposure