Download
1 / 50
500 likes | 559 Views
Learn about the challenges of intracranial pressure during neuroanesthesia procedures and the importance of effective management strategies. Discover the impact of various conditions on ICP and the principles of anesthesia for craniotomy surgery.

E N D
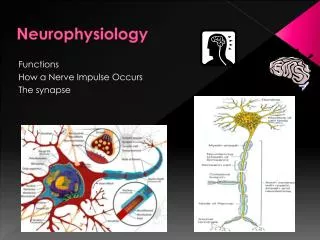
Neurophysiologyand Intracranial Hypertension Mani K.C Vindhya M.D Asst Prof of Anesthesiology Nova Southeastern University
Anesthesia for Craniotomy • Three major issues: • 1. ICP. The skull is a rigid container, so an increase in intracranial volume (ICV) tends to increase intracranial pressure (ICP). • 2. Glucose and oxygen supplyand demand. The brain has a high energyrequirement with no capacity to store substrates. • 3. Venous air emboli. Air can be entrained into cerebral veins, causing venous air emboli. This can happen any time the head is higher than the heart.
Three basic principles of anesthesia for craniotomy surgery • 1. Employ techniques to decrease intracranial volume (ICV) and intracranial pressure (ICP). • Maintain cerebral perfusion and oxygenation. • Monitor for sudden changes in vital signs (as would be caused by venous air emboli).
Introduction to Intracranial Hypertension • Intracranial pressure (ICP) is a main concern in many intracranial neuroanesthesia cases: • (Sulek CA.Intracranial Pressure, In: Cucchiara RF, Black S,Michenfelder JD, eds. Clinical Neuroanesthesia, 2nd ed., Churchhill Livingstone, New York, 1998, pp. 73-123.) • Brain tumors • Head injury • Subdural or epidural hematomas • Subarachnoid hemorrhage (ruptured aneurysm) • Arteriovenous malformation • Hydrocephalus
Many other disease processes can also increase ICP: (SulekCA, ibid.) • Stroke • Hypoxic injury • Pseudotumor cerebri (impaired CSF reabsorption) • Hepatic encephalopathy • Eclampsia • Venous sinus thrombosis • Inflammatory processes • Reye syndrome (cerebral edema in children after infection)
Why is intracranial pressure (ICP) a main concern in intracranial neuroanesthesia? 1.Skull = a rigid and non-compliant container. This is the Monro-Kellie doctrine or hypothesis (Katz J. Anesthesia for the patient with elevated intracranial pressure. ASA Refresher Course Lecture 152:1-7, 1988). 2. Any increase in intracranial volume (ICV) tends to produce an increase in intracranial pressure (ICP). 3.Not exactly a direct 1:1 relationship between ICV and ICP
Intracranial Volume-Pressure Relationship • Compliance = change in volume / change in pressure(Think pulmonary compliance) • Elastance = change in pressure / change in volume (The intracranialvolume-pressure relationship is usually expressed as an elastance curve.) • 3. With compensation, fairly large increases in ICV cause only a small increase in ICP. • 4. With decompensation, a further small increase in ICV causes a large increase in ICP.
Mechanisms that compensate for an increase in intracranial volume Decrease CSF volume in the intracranial vault • CSF is displaced into distensible spinal dural sac. • Decrease CSF production relative to reabsorption Decrease intracranial blood volume (especially in dural veins)
Decreasing ICP by decreasing ICV, shifting the ICP-ICV curve down to the left, is a main goal of intracranial neuroanesthesia.
Two main consequences of decompensation 1. Decreased cerebral perfusion pressure (CPP), resulting in cerebral ischemia. 2. Risk of herniation (Fishman RA. Brain edema. NEJOM 293: 706, 1975)
Decreased cerebral perfusion pressure (CPP), resulting in cerebral ischemia. CPP = MAP - ICP (or CVP, whichever is greater)
Clinical Presentation of Increased ICP • Acute vs. chronic process and location • Classic clinical manifestations: (Sulek CA, ibid.) • Headache • Nausea and vomiting • Visual disturbances • Altered mentation • Papilledema • Ocular palsies • Other symptoms with worsening ICP include: (Shapiro HM, Drummond JC. Neurosurgical anesthesia and intracranial hypertension.In: Miller RD (ed), Anesthesia, 3rd. ed. New York: Churchill-Livingstone, 1990, pp. 1737-9. ) • CNS - drowsiness, unconsciousness, decerebrate posturing • Cardiovascular (Bendo AA, Luba K. Recent Changes in theManagement of Intracranial Hypertension. International Anesthesiology Clinics 38 (4):69-85, 2000.) • Respiratory - abnormal breathing, apnea No clinical sign reliably indicates the ICP level.
Cardiovascular • Cushing’s response = systemic hypertension + reflex bradycardia • Cushing’s triad = intracranial HTN + systemic HTN + reflex bradycardia
Diagnosis of increased ICP Indirect diagnosis (CT scan, MRI). Findings suggestive of increased ICP include: (Bendo AA, Luba K, ibid.) • Midline shift • Obliteration of basal cisterns • Loss of sulci • Ventricular effacement (or enlargement, as with hydrocephalus) • Edema (region of hypodensity) • Direct measurement of ICP • Methods: • Subdural bolt • Subdural catheter • Epidural transducer • Intraparenchymal fiberoptic catheter • Ventriculostomy • Findings • Normal ICP < 10 mm Hg • Elevated ICP > 15 mm Hg
Components that Contribute to Intracranial Volume (ICV) and Intracranial Pressure (ICP)
Underlying Assumption Regarding Cerebral Blood Flow (CBF) and ICP • CBF = cerebral blood flow, CBV = cerebral blood volume, • ICV = intracranial volume, and • ICP = intracranial pressure
1. You’d assume that anything that increased CBF to the brain would be good. • 2. Actually, a large increase in CBF tends to increase ICP and squish the brain, so ultimately it is bad
Physiologic Control of Cerebral Blood Flow (CBF) • Normal global CBF • Average global CBF = 50 cc / 100 gm / min • Grey matter CBF = 80 cc / 100 gm / min • White matter CBF = 20 cc / 100 gm / min • CBF = approximately 750 cc / min in adult • Brain weight = 1.5 kg, about 2% of body weight • 15% of cardiac output
Major Factors in Physiologic Control of CBF Metabolic control -- CBF varies directly with brain activity and thecerebral metabolic rate of oxygen consumption, CMRO2. • Relationships
Glasgow coma scale • CMRO2 varies directly with Glasgow coma scale = a coma grading score used in head trauma (Obrist WD et al, J Neurosurg 61: 241-53, 1984; Frost EAM (ed), Clinical Anesthesia in Neurosurgery, 2nd ed, 1991, pp. 403-8)
Autoregulation • CBF changes in response to cerebral perfusion pressure (CPP) • Lower limit of autoregulation for CPP = 50 mm Hg • Upper limit of autoregulation = 150 mm Hg Lower limit of autoregulation for mean arterial pressure (MAP) is now being shown as 70 mm Hg
Arterial CO2 tension ("Chemical control") = CBF changes in response to paCO2
Arterial O2 tension ("Chemical control") = CBF changes in response to paO2
Effects of low CBF on the functional status and viability of neurons
Other Factors in Control of Cerebral Blood Flow (CBF) • Neurogenic Control • Autonomic N.S. • Sympathetic stimulation • Modest cerebral constriction • Decrease in CBF • Parasympathetic stimulation • Modest cerebral dilatation • Increase in CBF • Central neurogenic control (less well defined) • Noradrenergic pathways • Cholinergic pathways • Serotonergic pathways • Temperature • CBF changes directly related to brain activity andCMRO2
Temperature CBF changes directly related to brain activity and CMRO2
Temperature Effect of temperature reduction on CMRO2 (Miller et al, eds, Anesthesia, 4th ed, Vol. 1, p. 693):
Blood viscosity Effects of polycythemia and anemia
A decrease in Hgb causes a compensatory: 1) Increase in CBF (according to Poiseuille’s equation, a decrease in viscosity results in a decrease in resistance, and thus an increase in flow)R = 8Ln / (πr4) where R = resistance, L = vessel length, n = viscosity, r = radius 2) Decrease in O2 content (due to decreased Hgb) CaO2 = (1.39 x Hgb x FSaO2) + (0.003 x paO2) 3) Little change in O2 delivery until Hgb drops less than 7 O2 delivery = CBF x CaO2
Patient Position • Head down (Trendelenberg) • Increases jugular venous pressure • Decreases cerebral venous drainage • Head up (reverse Trendelenberg) • Decreases jugular venous pressure • Increases cerebral venous drainage
Rules to help remember values for physiologic control of CBF • "Rule of 50's" • 50 cc / 100g / min = normal global CBF • 80 cc / 100 g / min = grey matter blood flow • 20 cc / 100 g / min = white matter blood flow • 50 mm Hg = lower limit of autoregulation • for cerebral perfusion pressure (CPP) • 70 mm Hg = lower limit of autoregulation for MAP • 150 mm Hg = upper limit of autoregulation • 50% decrease in CBF = approximate change in CBF when you hyperventilate from paCO2 of 40 to 25 • 50 mm Hg = paO2 at which hypoxic vasodilatation starts to occur • 50% (actually 60%) = % of brain metabolic activity devoted to function (EEG activity) • ! 50% (actually 40%) = % of brain metabolic activity devoted to maintaining brain integrity (non-EEG, basal activity) • 50:50 = distribution of CSF in skull vs. around spinal cord
"Rule of 3's": • 3 = components inside skull that contribute to ICP: • Brain (neurons, extracellular fluid, and glia) = 85% • Cerebrospinal fluid (CSF) = 10% • Blood volume = 5% • ! 3 to 3.5 cc / 100 gm / min =CMRO2 (cerebral metabolic rate of oxygen consumption) • 3.5 cc / kg / min = BMR (basal metabolic rate) • Accordingly, 3.5 x 70 kg = approx. 250cc O2 / min • 3 minutes = approx. time to form 1 cc of CSF (in adults) • CSF formation rates: • 0.33 cc / min 20 cc / hour • 1 cc / 3 min 480 cc / day • 3X = CSF turnover in 1 day • 480 cc / 3X = 160 cc volume of CSF
Cerebrospinal Fluid (CSF) (Stoelting RK, Pharmacology and Physiology inAnesthetic Practice, 2nd ed., J. B. Lippincott Co., Philadelphia: 1991, p. 630.)1. CSF Formation: Choroid plexuses in cerebral ventricles, especially 2 lateral ventricles 2. CSF Reabsorption: Arachnoid villi in venous sinuses
Ways to Control Intracranial Hypertension • Decrease brain bulk • Mannitol • Mechanism: osmotic diuretic (as is hypertonic saline) • Dose: 0.25 to 1 gm/kg IV • Caution: Administer slowly over 10 min. Mannitol-induced hypotension could increase ICP. • Onset of action = 10-15 min • Duration. Effects on ICP last only 2-3 hours. • Furosemide • Mechanism: loop diuretic • Dose: 0.5 to 1 mg/kg alone or 0.15 to 0.3 mg/kg with mannitol • Cautions • electrolyte abnormalities • Hypokalemia may require K+ repletion. • Dexamethasone • Mechanism: decreases edema around some solid brain tumors (Skjoeth J, Bjerre PK. Acta Neurol Scand 96: 167-70, 1997). • Dose: 10-20 mg IV • Onset of action: Several hours or days to decrease ICP • Cautions: • Causes hyperglycemia • Steroid-treated head-injured patients have a worse out- come (Saul et al, J Neurosurg 54: 596, 1981; Dearden et al, J Neurosurg 64: 80, 1986).
Ways to Control Intracranial Hypertension • Decrease CSF Volume • Ventriculostomy • Lumbar drain • Decrease blood volume • Optimize hemodynamics (MAP, CVP, PCWP, HR) to maintain CPP. • CPP = MAP - ICP (or CVP, whichever is greater) • Avoid severe anemia • Avoid severe hypotension, resulting in cerebral ischemia. • Avoid severe hypertension, resulting in: 1) cerebral edema, 2) hemorrhage, or 3) herniation
Target normovolemia: Avoid under- or over-hydration. • No longer “run ‘em dry.” • For normal craniotomy, • Hourly maintenance + • Replace urine cc for cc + • Cover blood loss 3:1 with crystalloid • Avoid extreme hyperglycemia a. Assumption: If glucose = energy substrate for the brain, then an increase in plasma glucose should be beneficial. • b. Actually, elevated plasma glucose levels are deleterious in cerebral ischemia (Wass CT, Lanier WL. Mayo Clin Proc 71: 801-12, 1996). • In animal models, hypoglycemia at the onset of ischemia worsens outcome. • In humans, hyperglycemia is associated with a worsening of post-ischemia brain injury. • Why? Intracellular acidosis injures neurons and glia. • Common sense goals for glucose management: • Monitor glucose levels to maintain “normoglycemia” as rigidly as possible. • Avoid IV glucose infusions unless indicated.
NB: Drug infusions • Use lactated Ringer’s (LR) with caution. • Converted to glucose in the liver • Slightly hypotonic (vs. slightly hypertonic NSS) • “Big Miller recommends resuscitation with • NSS + LR (50:50) • Use insulin to treat hyperglycemia. • Don’t allow sustained glucose > 250 (“Big Miller”). • Avoid rapid fluid shifts, electrolyte abnormalities, and hypoglycemia • Optimize ventilation. • Reasonable goals: • paO2 > 100 mm Hg • paCO2 35 mm Hg • Avoid hypoventilation pre-op and intra-op. Hypoxia and hypercarbia increase CBF and ICP, resulting in brain swelling. • Hyperventilation on demand? • paCO2 of 25-30 may still be necessary if brain is “tight” • Never go below a paCO2 of 25. • Can cause cerebral ischemia due to cerebral constriction in some pathologic conditions (von Helden et al, Acta Neurochir Suppl Wien 59: 102-6, 1993. • Hyperventilation is only effective to decrease ICP for 6-8 hours
Temperature control • Avoid hyperthermia. • Increases brain metabolism, CMRO2, and CBF • Worsens outcome after cerebral ischemia in animal experiments (Minamisawa et al, Ann Neurol 28: 26- 33, 1990) • Intra-op moderate hypothermia (34-35 oC)? • Decreases ICP in head-injured patients by decreasing brain metabolism, CBF, CBV, and CSF production. • Multicenter IHAST trial tested if beneficial for intracranial aneurysm surgery (Hindman BJ et al, Neurosurgery 44: 23, 1999). • Published results of completed trial indicate no better outcome with hypothermia (33.5 oC) than normothermia (36.5 oC) (Todd MM et al, N Engl J Med 2005; 352:135-45.) • Position to improve cerebral venous return • Neutral position • Head up
Decrease Brain Bulk Mannitol Furosemide Dexamethasone (solid tumors) Decrease CSF Volume Ventriculostomy Spinal drain Decrease blood volume Optimize hemodynamics Target normovolemia Avoid extreme hyperglycemia Optimize ventilation Avoid hyperthermia Improve cerebral venous return Summary: Methods to Control Intracranial Hypertension