Download
1 / 20
200 likes | 442 Views
Appendicitis in Africa. ALC Jones Oct 2010. Case Presentation 1 . 20 western male 1 day history progressive para -umbilical pain moving to RIF Rebound and percussion tenderness Vomiting Rovsing’s + ve. Case Presentation – Investigation?. Observations – pulse 93, BP 120/79, t – 37.4C

E N D
Appendicitis in Africa ALC Jones Oct 2010
Case Presentation 1 • 20 western male • 1 day history progressive para-umbilical pain moving to RIF • Rebound and percussion tenderness • Vomiting • Rovsing’s +ve
Case Presentation – Investigation? • Observations – pulse 93, BP 120/79, t – 37.4C • Bloods – raised inflammatory markers • Neutrophilia (left shift) • Radiology? Xray, U/S, CT? • Diagnosis? - Appendicitis • Mesenteric adenitis, terminal ileitis, Meckel’sdiverticulum, lymphoma, renal colic, UTI, carcinoid, testicular torsion
Post-operatively • Antibiotics • E&D • Follow up?
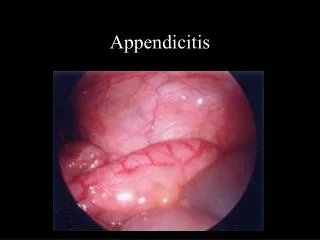
Aetiology and pathophysiology • Obstruction of the appendix lumen • Mucus production, swelling, decrease venous return,ischaemia, necrosis, perforation, peritonitis, death • Low fibre diet – faecal stasis
Squatting Hypothesis • “"When the thighs are pressed against the abdominal muscles in this position, the pressure within the abdomen is greatly increased, so that the rectum is more completely emptied. • Our toilets are not constructed according to physiological requirements. Toilet designers can do a good deal for people if they will study a little physiology and construct seats intended for proper [elimination].“ H. Aaron 1938
Case Presentation 2 • 26 male - Zulu farmer • 3 day history of ubuhlungu in lower abdomen. • Progressively worse, diarrhoea, anorexia • Feverish,oliguric • Lower abdomen generally tender with peritonism.
Case Presentation 2 • Observations – pulse 120, BP 65/30, t – 39C • Bloods – raised inflammatory markers • Cr – 230 U – 20 LFTS-NAD • Radiology? Xray, U/S, CT? • Diagnosis? - Gangrenous/Perforated Appendicitis • Yersinia, TB, Toxoplasmosis, Schistomiasis • UTI, Carcinoid, Testicular Torsion
Case Presentation 2 - Management • Resuscitation • IV abx • How quickly to theatre? • Surgical approaches • Post-op care • ?Histology follow up
Appendicitis in Africa • Lower incidence rates in rural population compared to urban and developed countries (?but rising) • Direct correlation between delayed presentation and perforation [2] • Atypical history – likely suppurative appendicitis. ?higher perf rates check histology [3]
Appendicitis in Africa • Studies have shown prolonged post-op stay – higher incidence perforation+ peritonitis • Africans have a higher DALY compared with developed countries
Case Presentation 3 • 43 female presents with 2/7 lower abdominal pain and vomiting • BNO. Pain localising in RIF. Tender with rebound and localised guarding. • Hb – 10.2 g/dl WCC -14 Neut – 11 • Plt – 253 Cr-122 U-12
Case Presentation 3 • On examination: Mass in RIF • Differential diagnosis?
Case Presentation 3 • Appendix Mass – management options • 1. Conservative – IV abx and 6-8 weeks interval appendix • 2. Immediate appendicectomy / Right hemi after several days of IV abx • 3. Totally conservative management
Summary • Incidence of appendicitis is generally less in developing continents ie. Africa, but rising • Treatment is more invasive as presentations are late and associated with higher rates of perforation and gangrene • Higher DALY • Consider other differential diagnosis and aetiology to appendicitis, hence always send for histology.
References • Jones BA, Demetriades D, Segal I, Burkitt DP (1985). "The prevalence of appendicealfecaliths in patients with and without appendicitis. A comparative study from Canada and South Africa". Ann. Surg. 202 (1): 80–2. • Chamisa I (Nov 2009) A clinicopathological review of 324 appendices removed for acute appendicitis in Durban, South Africa: a retrospective analysis. Ann. RCSEngVol 91, No 8, pp. 688-692(5) • Hobler, K. (Spring 1998). "Acute and Suppurative Appendicitis: Disease Duration and its Implications for Quality Improvement. Permanente Medical Journal • Ojo OS, Udeh SC, Odesanmi WO, Review of the histopathological findings in appendices removed for acute appendicitis in Nigerians. J R CollSurgEdinb. 1991 Aug;36(4):245-8. • ES Garba, A Ahmed. (2008)Management of appendiceal mass. Ann Afr Med Vol 7 (4) p200-204 • World Health Organisation