Download
1 / 53
620 likes | 1.79k Views
by Chanda McDaniel 1/08. Appendicitis. Objectives. To review 3 cases of appendicitis (that presented to AUCC at DH) To discuss how we could improve the care of these patients To review the presentation, work-up, and differential diagnosis of appendicitis. Case 1 HPI.

E N D
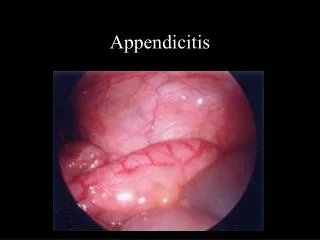
by Chanda McDaniel 1/08 Appendicitis
Objectives • To review 3 cases of appendicitis (that presented to AUCC at DH) • To discuss how we could improve the care of these patients • To review the presentation, work-up, and differential diagnosis of appendicitis
Case 1 HPI 37yo female presents to PCP (seen by resident) for 6 wk postpartum check up with abdominal pain x 5-7 days. No N/V. Pain is achy/diffuse. Subjective fever yesterday. No appetite. Drinking. Nl BMs. No dysuria or abnormal vaginal discharge. Stopped bleeding 1 ½ weeks ago.
Case 1 Physical 37.5 128 124/81 22 NAD H - RRR w/o M A - TTP midline, RLQ, LLQ, NABS, soft, non-distended, + guarding Pelvic - midline tenderness, no adnexal tenderness, no foul-smelling discharge
Case 1 Labs U/A-1.025, pH 5, 1+pro, 1+Hgb, 1-5 WBCs, 6-10 RBCs UHCG - negative
Case 1 PCP Dx, Plan Late postpartum endometritis Doxycycline 100mg po BID x 14 days Vicodin, Colace, Ibuprofen RTC 1 week
3 days later Pt presents to AUCC with worsening abdominal and low back pain. Dizzy. Decreased appetite. Fever. Pain 5/10. Nausea x 1 wk. No emesis, diarrhea, dysuria, vaginal discharge or URI sxs.
AUCC Physical 38.3 113 16 113/70 99% RA HEENT – pale conjunctiva, nl o/p H – RRR w/o M (90) L – CTAB A – NABS, soft, tender in suprapubic area, less in RLQ, no rebound, no obturator or psoas sign GU – no CMT, min. discharge, uterus TTP
AUCC Labs/xray UA – 1-5 WBC, 1-5 RBC, 1+ bacteria WBC 12.6, Hb 12.5, Hct 38.9, plts 323 Chem 7 – nl, Calcium – nl Pelvic US – nl CT – 9.6x7cm mass abuts cecum with surrounding fat stranding most likely perforated appendicitis with associated abscess
AUCC course Pt seen by surgery who wanted to admit & take pt to OR. She refused and left AMA, but said she would return in AM. Pt returned the next day and said that she refused admission due to a religious holiday and was admitted to surgery. She was discharged on Levo and Flagyl post op.
Endometritis Most cases develop within the 1st week after delivery 15% present between 1-6 weeks postpartum May present as late postpartum hemorrhage Clinical criteria Fever and uterine tenderness occurring in a postpartum woman foul lochia, chills, and lower abdominal pain Admit for IV antibiotics (Clinda/Gent)
What could we (at DH) have done differently? PCP could have considered appendicitis in the differential Pt presentation was atypical for endometritis Late onset No VB or discharge Abnormal vitals (HR 128) not addressed No labs were drawn (even for baseline) Needed admission/IV Abx (?), if diagnosis of endometritis was correct
Case 2 HPI 21 yo female presents with abd. pain and vaginal bleeding x 3 days. Not using pad – just on TP. Recently had IUD removed. No N/V. PMH – Depression Meds – Prozac NKDA
Case 2 Physical 36.3 119 110/63 18 NAD Chest – clear H – RR A – soft, marked tenderness in RLQ, tender in suprapubic area & LLQ, no rebound, NABS Pelvic – blood in vault, cervix/uterus tender, adnexa tender R>L
Case 2 Labs UA – mod ketones, 1.015, 2+pro, tr blood, tr leu, 11-20 WBC, no RBC, 1+crystals UHCG – negative CBC – WBC 26.6, hb 14.9, hct 42.9, plt 406, 87% segs Chem 7 normal except Na 133
Case 2 Dx & Plan Abdominal pain with elev. WBCs, some WBCs in urine R/O PID vs UTI, doubt appy Urine cx P Gonorrhea/Chlamydia P Levofloxacin 500mg BID, Flagyl 500mg BID x 14 days
Case 2 AUCC f/u Seen 1 day later in AUCC – “Pt did not want CT yesterday. Feels better.” Meds upset stomach. Ate some breakfast. No nausea now. VS 38.4 113/69 124 20 A - +BS, soft, tender in RLQ w/ guarding WBC 20.7, Hb 13.7, Hct 40.2, Plts 333 CT – RLQ 11x4cm abscess, adj to cecum
Case 2 Hosp. course Pt admitted for perforated appendix (approximately 7-10 days old) and placed on IV Timentin. IR placed drain on hosp. day 1 and removed on day 7 after 2nd CT scan (although I can’t find the report of 2nd CT). Discharged on Augmentin, Colace, Vicodin.
What could we have done differently? If appendicitis was in the differential and it was not visualized on US consider CT or surgery consult. If patient refused CT, we could have improved our documentation on her initial visit.
Case 3 HPI 51 yo male with epigastric pain since this am. N/V x 3. No diarrhea. No fever. PMH – No hospitalizations. Meds – Tylenol flu All – none SHx – no exposures, ETOH yesterday
Case 3 Physical 36.7 142/85 66 20 (not orthostatic) General - Alert, NAD HEENT – NCAT, anicteric, o/p -, neck supple w/o LAD H – RRR w/o m L – CTAB A – NABS, soft, mild epigastric tenderness to palpation, more TTP in RLQ, + rebound, - heel tap, - obturator, + psoas, nl rectal
Case 3 Labs WBC 16.4, Hb 16.1, Hct 47.8, Plts 221, 91% Segs Chem 7 – normal LFT’s – normal Amylase – 27 U/A – 1.038, 2+pro, 1+Hb, 2+glc, - WBC, - RBC Guaiac - negative
Case 3 CT Verbal report – Equivocal for appendicitis Written report – There is considerable fecal material within the cecum, but the terminal ileum is not dilated and the appendix is normal. Moderate thickening of sigmoid colon, which may indicate a prior inflammatory process. No evidence of acute diverticulitis.
Case 3 Surgery Consult 51 yo w/ epigastric pain – better now. N/V x 1. A – NTTP CT – poorly visualized appendix A/P – resolved Abd pain, with elevated WBC. Would like to admit for obs, but pt would like to go home. Return to AUCC in am for recheck, CBC.
Case 3 AUCC f/u 51 yo w/ abd pain seen yesterday. N/V x2 this am. Constant pain. No appetite. 37.3 64 20 128/74 A – RLQ tenderness WBC 20.3, Hb 15.7, Hct 46, plts 225, 87S Admitted to surgery. Laproscopic eval –> partially necrotic appendix (ruptured per path) open appendectomy. Discharged on Levo/Flagyl.
What could we have done differently? Talked pt into staying the night in the hospital? This may have prevented rupture?
Appendicitis Epidemiology 250,000 cases/yr in US most common in 2nd/3rd decades of life highest incidence in 10-19 yo age group no age is exempt males > females rate of negative appendectomies (15-20%) has not declined in the last 15 years despite the increasing use of US and CT DH: 1-2 carcinoids, 2-3 parasitic infections, TB, TOA/several hundred surgeries (<1%) Mortality <1% (nonperf), >5% (perf)
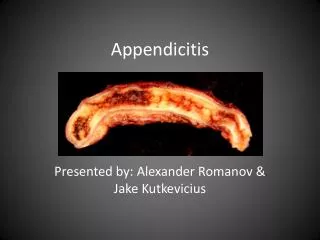
Pathophysiology 1) Obstruction of lumen young = lymphoid follicular hyperplasia (due to viral or bacterial infection and dehydration) older = fibrosis, fecalith, neoplasm 2) Fills with mucusdistendsincreases intraluminal pressurethrombosis ischemianecrosis (<24hrs) and perforation (>48hrs)
Organisms E. coli Peptostreptococcus Bacteriodes Fragilis Pseudomonas
Appendix Anatomy normal = lies in RLQ retrocecal (65%) pelvic (30%) intestinal malrotation = LUQ pregnant = RUQ
Symptoms Initial indigestion flatulence bowel irregularity Epigastric or periumbilical pain visceral - constant, not very severe in intensity, poorly localizable Then, N/V (not usually 1st symptoms) Fever (higher suggests perf) Sxs may subside (temporarily) after rupture
Abdominal Pain Visceral Parietal Referred
Visceral pain Stretching, distention, torsion, or contraction of abdominal organs Carried on slow-conducting fibers Dull ache Location correspond to dermatomes that match the innervation of the injured organ Epigastrium organs proximal to ligament of treitz (hepatobiliary, spleen) Periumbilicalligament of treitz to hepatic flexure of colon Midline lower abdorgans distal to hepatic flexure
Parietal Pain Well-localized Results from direct irritation of the peritoneal lining A delta fibersrapid conduction Sharp pain sensation
Referred pain Occurs when visceral afferents carrying stimuli from a diseased organ enter the spinal cord at the same level as somatic afferents from a remote anatomic location. Typically well-localized Gall bladder inflammation to R shoulder Diaphragmatic rupture to shoulder Heart attack to L arm
Physical Exam: Appendicitis Pain is subjective Tenderness is objective; local tenderness in RLQ McBurney’s point (1/3 of distance of line from anterior iliac spine to umbilicus) May have tenderness in RLQ during rectal and pelvic
Common Signs of Appendicitis • Right lower quadrant pain on palpation (the single most important sign) • Low-grade fever (38°C [or 100.4°F])--absence of fever or high fever can occur • Peritoneal signs • Localized tenderness to percussion • Guarding • Other confirmatory peritoneal signs (absence of these signs does not exclude appendicitis) • Psoas sign--pain on extension of right thigh (retroperitoneal retrocecal appendix) • Obturator sign--pain on internal rotation of right thigh (pelvic appendix) • Rovsing's sign--pain in right lower quadrant with palpation of left lower quadrant • Dunphy's sign--increased pain with coughing • Flank tenderness in right lower quadrant (retroperitoneal retrocecal appendix) • Patient maintains hip flexion with knees drawn up for comfort
3 PE findings with highest predictive value of appendicitis 1) RLQ pain 2) Abdominal rigidity 3) Migration of a pain from periumbilical region to the RLQ Occur in about 50% of patients
Retrocecal appendix Appendix doesn't touch parietal peritoneum Sxs not localized dull ache +psoas sign flank pain
Psoas sign Inflamed appx is in retroperitoneal location in contact with psoas
Pelvic Appendix May have no abdominal signs Urinary frequency Dysuria Tenesmus Diarrhea Tenderness with rectal exam Positive obturator sign
Obturator sign Inflamed appx is in pelvis, in contact with obturator muscle
Labs UA r/o UTI (micro hematuria/pyuria in 30% appys) >30 RBC or >20 WBC - urinary UHCG r/o ectopic Pelvic cultures CBC leukocytosis 30% have normal WBC (95% have left shift)
Radiology (CT or US) Obtain if diagnosis is unclear. A population based study suggested that the rates of negative appendectomies have not changed between 1980 and 1999.
CT Appy Sensitivity 94% Specifity 95% Air or contrast in appendix – excludes dx Diameter 6 mm or less - normal Non-visualized appx does not rule out appendicitis If pt with sxs for a short duration, only min. inflammation may be present IV contrast (?) - may improve wall appearance/inflammation
Appendicitis on CT Dm >6mm Appendicolith Cecal thickening Arrowhead sign abscess formation cecal thickening
Arrowhead sign An axial CT image in the upper pelvis shows edema of the cecal wall which, along with barium in the cecum (C), contributes to the "arrowhead sign" of appendicitis. A dilated fluid filled appendix (large arrow) is seen with adjacent stranding of retroperitoneal fat (arrowheads). The appendix follows a retrocecal course (small arrows).
CT radiation “There is direct evidence from epidemiologic studies that the organ doses corresponding to a common CT study (2-3 scans, dose 30-90 mSv) result in an increased risk of cancer.” 10,000 adults, 35 yrs old, US instead of CT Appendicitis would be missed in 480 cases 2 patients could be prevented from developing cancer in the future