Download
1 / 18
200 likes | 599 Views
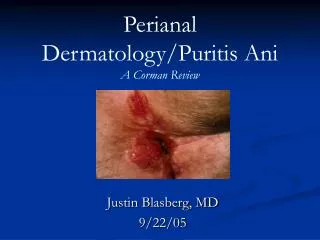
Perianal mass. 54 year old Known diabetic. History of present illness. One day PTA Painful sensation at anal region after passing out hard stool 2 days PTA patient felt a soft mass over the perianal region which was painful to touch Few hours PTA

E N D
54 year old • Known diabetic
History of present illness • One day PTA • Painful sensation at anal region after passing out hard stool • 2 days PTA • patient felt a soft mass over the perianal region which was painful to touch • Few hours PTA • patient started to experience painful sensation on the anal region which was aggravated when assuming sitting position
Review of system • No dysuria, no frequency • No change in bowel habit • No nausea nor vomiting • No weight loss
Past medical history • IDDM3 • Family history • (-)HPN, CA • (+)DM
Physical exam • BP-120/80, PR-85/min, RR-18/min, T-37.8°C • HEENT: anicteric sclerae, pink palpable conjuctivae • Heart&lungs: unremarkable • Abdomen: flat, soft, nontender with normoactive bowel • DRE: erythematous, warm, tender 5x4cm mass at right perianal region *DRE cannot be tolerated by patient
Differential diagnosis tim, eto parang wag na nating isali kasi hindi naman pasok sa patient natin..?sa tingin mo?
assestment • Thrombosed external hemorrhoids • Anorectal abscess i changed my mind.. thrombosed internal hemorrhoids nga... pero nagawa ko na ung anorectal abscess.. nlagay ko nalang din..
Thrombosed external hemorrhoids • distended vascular tissue in the anal canal distal to the dentate line • present with pain on standing, sitting or defecating • usually develop over time and may result from straining with stools, childbirth, lengthy car trips or prolonged sitting, constipation or diarrhea
Anorectal abscess • More common in M>F • Peak incidence 30-50y/o • Prevalent in immunocompromised like diabetics, IBD & HIV positive • Recurrent perianal infection
Presentation and evalutation • Perianal pain • Fever • Difficultyu voiding • Bloody stool • On PE, large fluctuant area is readily visible
40-50% - perianal • 20-25% - ischiarectal • 2-5% - intersphincter • 2.5% - supralevator
Anatomy & physiology • Abnormal fluid containing cavity in the anorectal rtegion • Results from infection involving the glans surrounding the ana canal • When stool accidentally enters the anal glands, the glands become infected and an abscess develops
Management • Uncomplicated • Small incision close to anal verge is made & a malienkat drain in advanced into abscess cavity • Complicated • Should perform in OR under anesthesia • Antibiotics at least 2 weeks