Download
1 / 40
560 likes | 5.03k Views
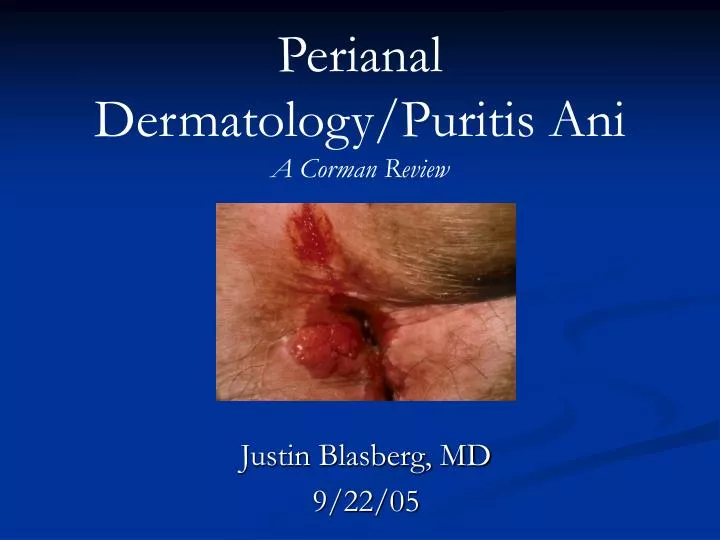
Perianal Dermatology/Puritis Ani A Corman Review. Justin Blasberg, MD 9/22/05. What to look forward to?. Description of skin conditions affecting the perianal area Review of the differential diagnosis Examples of common and uncommon findings Treatment of the relevant diseases.

E N D
Perianal Dermatology/Puritis AniA Corman Review Justin Blasberg, MD 9/22/05
What to look forward to? • Description of skin conditions affecting the perianal area • Review of the differential diagnosis • Examples of common and uncommon findings • Treatment of the relevant diseases
Classification of Skin Conditions • Inflammatory • Infectious • Neoplastic
Inflammatory • Pruritus ani • Psoriasis • Lichen planus • Lichen sclerosus et atrophicus • Atrophoderma • Contact (allergic) dermatitis • Seborrheic dermatitis • Radiodermatitis • Behcet’s syndrome • Lupus erythematosus • Dermatomyositis • Scleroderma • Erythema multiforme • Familial benign chronic pemphigus (i.e. Hailey-Hailey) • Pemphigus vulgaris • Cicatricial pemphigoid
Infectious Nonvenereal: • Pilonidal sinus • Suppurative hidradenitis • Anorectal abscess and anal fistula • Crohn’s disease • TB • Actinomycosis • Fournier’s gangrene • Ecthyma gangrenosum • Herpes Zoster • Vaccinia • Tinea cruris • Candidiasis • “Deep” Mycoses • Ambebiasis cutis • Trichomoniasis • Schistosomiasis cutis • Bilharziasis • Oxyuriasis (i.e. pinworm, enterobiasis) • Creeping eruption (i.e. larva migrans) • Larva currens • Cimicosis (i.e. bedbug bites) • Pediculosis • Scabies
Infectious Venereal: • Gonorrhea • Syphilis • Chancroid • Granuloma inguinale • Lymphogranuloma venereum (Chlamydia infection) • Molluscum contagiosum • Herpes genitalis • Condylomata acuminate
Neoplastic • Acanthosis nigricans • Leukoplakia • Mycosis fungoides • Leukemia cutis • Basal cell carcinoma • Squamous cell carcinoma • Malignant melanoma • Bowen’s disease • Extramammary Paget’s disease
Pruritus Ani • “itching in the anal area” • Symptoms: • Itching of anal and genital areas • Worsening at night • May awaken the patient from sleep • Scratching with exacerbation of complaint • Chronic itching can lead to atrophic or hypertrophic skin, with associated nodularity and scarring
Pruritus Ani Differential • Hemorrhoids • Anal fissure • Scarring from prior anal surgery • Constipation/diarrhea • Contact dermatitis • Mycoses • Seborrhea • Diabetes • Pinworm • Psoriasis • Neurodermatitis
Why me, why now? • Increased anal sphincter relaxation in response to rectal distension • Abnormal rectoanal inhibitory reflexes and a lower threshold for internal sphincter relaxation
Evaluation • Anoscopy and proctosigmoidoscopy • Magnifying lens • Woods lamp • Skin scrapings • Stool assessment?
What you might see • Marked edema with papillomatosis and nodularing resulting from chronic abrasion
Treatment • Injections of local anesthetics, phenol, and alcohol • Methylene blue • Diet modification • Sterilization? • Antibiotics?
Psoriasis • Chronic inflammatory disease of the skin • Characterized by rounded circumscribed erythematous dry scaling patches covered by grayish white or silvery white scales • Predilection for scalp, nails, extensor surfaces or limbs, elbows, knees, and sacral regions • Butterfly distribution over the coccyx and sacrum
Treatment • Moisturizers and agents with salicylic acid • Topical corticosteroids • Coal tar • Anthralin • Retinoid • Vitamin D3 derivatives • Ultraviolet B light • PUVA treatment • Methotrexate and Cyclosporine
Lichen Planus • Eruption of small, flat-topped papules with a distinct violaceous color and polypoid configuration • Found in flexor surfaces, mucous membranes, genitalia, and perianal area • Focal thickening of the granular layer, degeneration of the basement membrane and basal cells, and a bandlike lymphocytic infiltrate in the upper dermis • Diagnosis made with skin biopsy • Treatment with corticosteroids and occlusive dressings
What you might see • Moderate hyperkeratosis, thickening of the stratum granulosum, saw tooth configuration of rete ridges, and lymphocytic infiltration
Irritant and Contact Dermatitis • Irritant: Nonallergic reaction following exposure to an irritating substance • Alkalis, acids, metal salts, dusts, gases, and hydrocarbons • Allergic (contact): Allergic sensitivity to a number of responsible agents, also known as hypersensitivity of the delayed type (cell mediated hypersensitivity) • Dyes, oils, resins, chemicals used on fabrics, cosmetics, insecticides
Radiodermatitis • Secondary to radiotherapy of the rectum, anus, and prostate • Cell mitosis is arrested; skin change results from the dosage of radiotherapy • Erythema, edema, ulceration, and symptoms of burning, itching, or severe pain • Treatment with oral Vitamin A 8000IU BID • Hyperbaric O2 has also been found to be helpful
What you might see • Fibrosis of the dermis with sclerosis, atrophy of the epidermis, and absence of skin appendages
Pilonidal Sinus • Common infective process occurring in the natal cleft and sacrococcygeal region • Affects young adults and teenagers • 3:1 male predominance • Epithelium lined sinus is usually found to contain hair • Sinus may become infected, usually after puberty, with drains openings overlying the coccyx and sacrum • Infected abscess may extend to the perianal area that may be mistaken for an anal fistula
Why me, why now? • 2 Theories of formation: • Failure of fusion in the embryo, with entrapment of hair follicles in the sacrococcygeal region • Result of trauma, with the introduction of hair shafts into the subdermal area
Symptoms • Pain, swelling, purulent drainage at and around the site of the pilonidal opening • Typical appearance of an abscess may be evident • Fever and leukocytosis may be present
What you might see • Multiple openings overlying the sacrum and buttocks
What you might see • Indolent, granulating, nonhealing wound of a recurrent (persistent) pilonidal sinus
Treatment • Antibiotics? • Adjuvant to a surgical procedure • I&D • Definitive therapy: • Excision, excision with grafting or with an open wound to close secondarily, cryosurgery, and injection of sclerosing agents
Tuberculosis • Confused for Crohn’s, actinomycosis, anal fistula, colloid carcinoma, sarcoidosis, other skin conditions • Anal fistula is the most frequent presentation • Lesion appears as brownish red papule that can progress to an ulcerating plaque • Anal fissure in an unusual location that is slow to heal should raise the suspicion • Treatment: anti-TB drugs with resolve usually in 2 to 3 weeks
STD’s • Gonorrhea • Chancroid • Chlamydia • Herpes Simplex • Syphilis: • Chancre • Condylomata lata
What you might see • Large perianal mucoid warty mass composed of smooth-surfaced lobules
Neoplastic • Premalignant Lesions • Acanthosis Nigricans-ominous association with abdominal cancer • Affects face, neck, axillae, external genitalia, groin, inner thighs, umbilicus, and anus • Grayish velvety thickening or roughening of the skin • Epidermal papillomatosis, hyperkeratosis, and hyperpigmentation • Treatment is directed to the primary malignant condition
Premalignant Lesions • Leukoplakia • Whitish thickening of the mucous membrane epithelium occurring in patches of diverse size and shape • Seen in the anal canal • Associated with an increased risk of malignancy/epidermoid carcinoma • Symptoms of bleeding, discharge, and pruritic symptoms are the most common complaints • Hyperkeratosis and squamous metaplasia
Skin Cancer • Basal Cell Carcinoma • Most common cutaneous malignancy, extremely rare in the anal area • Tumors usually between 1-2 cm • Presents with a lump or ulcer • Bleeding, pain, pruritis, and discharge may be present • Treat with local excision and adequate margins • APR resection is performed for extensive or infiltrating tumors
What you might see • Ulcerating tumor has a pearly border
Skin Cancer • Squamous Cell/Epidermoid carcinoma • Tumor appears superficial, discrete, and hard • Ulcerates with progression • Mets to regional lymph nodes can occur • Treat with wide local excision
What you might see • Ulcerating friable tumor is noted
Bowen’s disease • Intraepidermal squamous cell carcinoma that spreads intraepidermally • Precursor to squamous cell carcinoma of the anus • Associated with HPV infection • Itching and burning, pain and bleeding • Treatment wide local excision with frozen section to ensure adequate margins
What you might see • An indurated erythemato-squamous patch involving the perianal area
Extramammary Paget’s Disease • Large, round, clear-staining cells with large nuclei • Symptoms of ulceration, discharge, pruritis, and occasionally bleeding and pain • Treatment depends on the presence/absence or underlying invasive carcinoma • Use of retinoid, etretinate, may benefit when there is no invasive carcinoma • More infiltrating disease an APR may be needed, otherwise wide local excision with grafting should be adequate for noninvasive disease
What you might see • Irregular but well-marginated erythematous erosive patch with slightly indurated edges
Extramammary Paget’s Disease • Stage I-localized perianal disease without carcinoma-tx with wide local excision • Stage IIA-localized disease without underlying malignancy-tx with wide local excision • Stage IIB-localized dx with associated anorectal carcinoma-tx with APR • Stage III-associated carcinomatous spread to regional lymph nodes-tx with APR plus chemoradiation, possible radical inguinal node dissection • Stage IV-distant mets-tx with standard palliative cancer management