Download
1 / 21
230 likes | 329 Views
Ascites and Hepatocellular carcinoma. Curtis Barry, MD UMASS ECHO April 21, 2017. Ascites. The Development of Ascites Revised Underfill. Peripheral vasodilation occurs as the result of decreased hepatic clearance of vasodilators such as glucagon and NO

E N D
Ascites and Hepatocellular carcinoma Curtis Barry, MD UMASS ECHO April 21, 2017
The Development of AscitesRevised Underfill • Peripheral vasodilation occurs as the result of decreased hepatic clearance of vasodilators such as glucagon and NO • The body compensates for the perceived drop in circulating blood volume in two ways: • increased cardiac output • activation of the renin-angiotensin system resulting in increased renal retention of sodium and free water
INITIAL WORKUP OF ASCITES: DIAGNOSIS PARACENTESIS Initial Workup of AscitesDiagnostic Paracentesis Optional Glucose, LDH Amylase Protein/Albumin Routine ? secondary infection ? cirrhotic ascites ? pancreatic ascites PMN count Culture Cytology ? malignant ascites ? SBP
Serum Ascites Albumin GradientSAAG • Best test for classifying ascites into portal hypertensive (SAAG >1.1 g/dL) and non–portal hypertensive (SAAG <1.1 g/dL) causes.
DIAGNOSTIC PARACENTESIS Diagnostic Paracentesis Indications • New-onset ascites • Admission to hospital • Symptoms/signs of SBP • Renal dysfunction • Unexplained encephalopathy Contraindications • None
The Management of Ascites • Dietary measures • Diuretics • Spironolactone • Large volume paracentesis • TIPS • Peritoneovenous shunt • Liver transplantation
Patient • 72 year old male with reported history of cirrhosis due to alcohol. Hasn’t seen a provider in many years presents for a new patient appt.
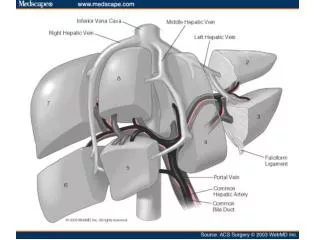
Dual Blood Supply of Liver HCC Diagnosis • The vascular supply of HCC arises from the hepatic artery through neovascularization. • Imaging of the liver has to be performed in a triple phase manner to account for the early arterial phase followed by the portal venous phase and the delayed phases Yu JS, et al, Am J Roentgenol 1999
Why HCC is Rising? HCC Epidemiology Why HCC is Rising? Increasing prevalence of patients with cirrhosis • Rising incidence of cirrhosis • HCV (main reason) • HBV • Other (?NAFLD/insulin resistance) • Improved survival of patients with cirrhosis El-Serag HB, Gastroenterology 2004
Dynamic Imaging Studies 4 Phase Liver CT Quick and easy 1/3 price of MRI Dynamic Contrast Enhanced MRI Longer and more Expensive Different images Biopsy only if imaging NOT “Classic” for HCC
Washout in HCC Washout in HCC HCC Diagnosis Arterial phase 2-min delayed Arterial phase 5-min delayed
Resection versus Transplantation HCC Treatment Resection versus Transplantation • TRANSPLANTATION • curative in early stage • advanced cirrhosis • shortage of donor livers • drop-out while awaiting transplantation • higher post-operative mortality; significant morbidity from recurrent hepatitis C • RESECTION • readily available • compensated cirrhosis without significant portal hypertension • high rate of recurrence of HCC
Radiofrequency Ablation for Hepatocellular Carcinoma HCC Treatment Probe insertion Deployment of tines and treatmentof tumor and surrounding region
Radiofrequency Ablation HCC Treatment
Trans-arterial Chemoembolization for Hepatocellular Cancer HCC Treatment
Systemic Therapies for Hepatocellular Cancer HCC Treatment Systemic Therapies for Hepatocellular Cancer • Only Sorafenib is currently approved • Taken orally • Compared to placebo increased overall survival by 37%, which calculated out to 2-3 months for pts with advanced HCC and COMPENSATED cirrhosis. • Main side effects are diarrhea, fatigue and rash on the hands and feets • Other medications are currently being investigated Mazzaferro V, et al, NEJM 2008
Patient • US ordered found to have 3.7cm lesion • MRI 4.8cm lesion • Treated with TACE • Listed for liver transplant