Download
1 / 21
220 likes | 495 Views
B alloon-pump assisted C oronary I ntervention S tudy BCIS-1. Simon Redwood. Divaka Perera , Rod Stables, Martyn Thomas. Disclosure Statement of Financial Interest. This trial was supported by unrestricted grants from: Datascope Eli Lilly Cordis. Current Indications for IABP.

E N D
Balloon-pump assisted Coronary Intervention StudyBCIS-1 Simon Redwood DivakaPerera, Rod Stables, Martyn Thomas
Disclosure Statement of Financial Interest This trial was supported by unrestricted grants from: Datascope Eli Lilly Cordis
Current Indications for IABP During High-Risk PCI ACC/AHA 2001 guidelines for PCI, JACC 2001, 37(8)2239 i-lxvi “… reserved only for patients at the extreme end of the spectrum of hemodynamic compromise… … it should be noted that in patients withborderline hemodynamics,ongoing ischemia, or cardiogenic shock, insertion of an intra-aortic balloonjust prior to coronary instrumentation has been associated with improved outcomes” ACC/AHA/SCAI Practice Guidelines Update 2005 “ Elective high-risk PCI can be performed safely without IABP or CPS in most circumstances …. Emergency high-risk PCI such as primary PCI can usually be performed without IABP or CPS…”
Current IABP use : Benchmark Registry CABG 17% Cardiogenic Shock 27% VSD / MR 12% High Risk PCI Non Shock 28% Angina / LVF / VT 16% Stone et al 2003, JACC 41(11) 1940-5
Elective vs provisional IABP in high-risk PCI 133 pts EF <30, elective PCI Group A: elective IABP, 61 pts. JS 8.0 + 2.8 Group B: Provisional IABP, 72 pts. JS 6.7 + 2.4 (p=0.008) Jeopardy score: coronary tree divided into 6 segments: LAD, D1, Cx, OM, RCA, PDA. 2 points for each lesion + 2 for each vessel distal to lesion Briguori et al, AHJ 2003;145:700-7
P = 0.02 P<0.001 IABP Use in High-Risk PCI N = 114 Elective PCI Non-Randomized 68 Prophylactic 48 Rescue IABP Mishra et al, Am J Cardiol 2006
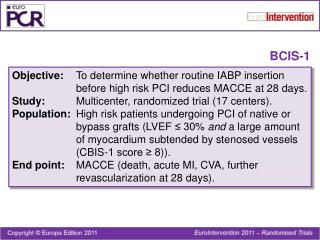
Balloon-pump assisted Coronary Intervention Study Objectives: To compare the efficacy and safety of elective Intra-Aortic Balloon Pump (IABP) insertion prior to high-risk PCI vs. conventional treatment (with no planned IABP use) Structure: Prospective, open, randomised trial 15-20 UK centres + 4 Polish centres n=300 (150 in each arm) Predicted MACE of 5% v 15%, 274 pts 80% power, sign 5%
BCIS-1 • Primary Outcome Measure • Major Adverse Cardiovascular Events at hospital discharge or 28 days(whichever is sooner), including • All-Cause Death • Acute MI (CKMB > 3xULN) • Further revascularization by PCI or CABG • CVA
Secondary Outcome Measures • Six month mortality • Procedural Complications • VT/VF requiring cardioversion • cardiac arrest requiring CPR/ventilation • prolonged hypotension (including IABP insertion in “No planned IABP” group) • Procedural success • Bleeding complications • Vascular complications • Duration of hospital stay
Inclusion Criteria • Impaired LV function (EF<30%) • Extensive Myocardium at Risk • LMS lesion • Jeopardy Score > 8 • Exclusion Criteria • Cardiogenic Shock • Acute STEMI within preceding 48hours • VSD, MR or intractable VT/VF • Contraindications to IABP insertion
Jeopardy Score Coronary tree divided into 6 segments: LAD, D1, Cx, OM, RCA, PDA. 2 points for each lesion + 2 for each vessel distal to lesion 2 2 2 2 2 2
0 BCIS-1 Polish Centres National Co-ordinator Dr Pawel Buszman
BCIS-1 Recruitment Completed 21st Jan 09 Total 301 patients
Unajudicated Clinical Events to Discharge/ 28 days LOS Median 2 days
Summary The exact role of haemodynamic support for high-risk PCI is unclear BCIS have designed and completed the first randomised trial of elective vs ‘bailout’ IABP in patients with poor LV function and severe coronary disease Full trial results due Q3 2009
Definition of Myocardial Infarction In BCIS-1 CKMB ≥ 3 X ULN.No ECG changes or symptoms are required Patients with admission MI CKMB ≥ 50% of pre-procedure value Patients with MI 24 hrs after CABG either a) the CKMB value ≥ 5 X ULN and new Q waves b) CKMB ≥10 X ULN (with or without Q waves), no symptoms are required Patients who die but no cardiac markers are available Presence of new ST segment elevation and new chest pain For all other circumstances, standard ESC/AHA definitions apply