Download
1 / 25
260 likes | 448 Views
Indoor Air Pollution Inequalities and Respiratory Health Risks: A Case Study in the Delhi City, India. Indoor Air Quality (IAQ).

E N D
Indoor Air Pollution Inequalities and Respiratory Health Risks: A Case Study in the Delhi City, India
Indoor Air Quality (IAQ) It refers to the nature of the conditioned (heat/cool) air that circulates throughout space/area, where we work and live i.e. the air we breathe most of the time (almost 80% of the time)
The Unacceptable IAQ "Air in an occupied space in which there are contaminants in concentrations leading to exposure that pose a significant health risk"
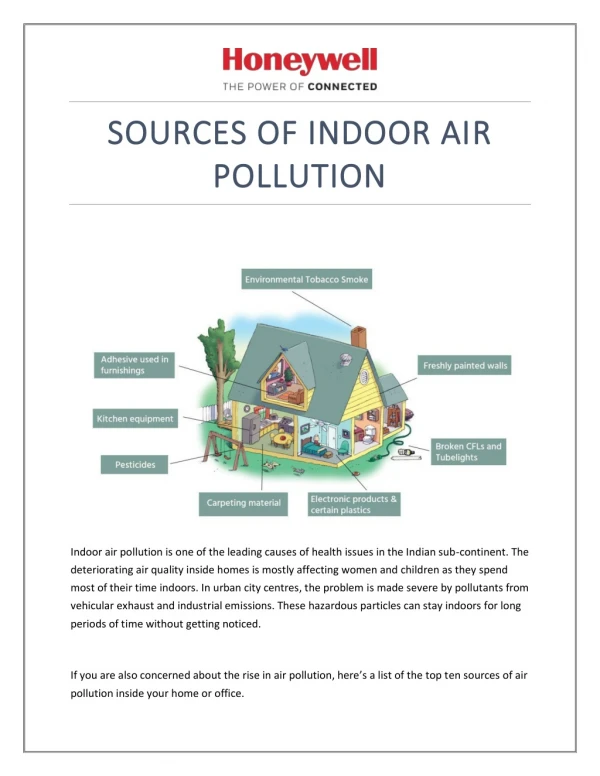
Factors affecting IAQ Societal Factors Urban rich Urban poor Engineering factors Ventilation design Poorly functioning cooking stoves Fuel type
Inequality in IAQ Disparity in income levels Fuel quality Dwelling types
Community Sensitization ProcessCommunity Participation (Brager et al,1973)
Participant’s actions in present study • The community profiles -Quantitative data on ambient pollution levels, housing characteristics and health performance were collected on site with the help of the supervisor of the railway division. Maps used as ready reference. • Enablingaction–Local residents were motivated, recruited and trained as interviewers. A sense of community ownership, confidence and acceptability was secured.
Plan of action-The local Residential Welfare Association approves the action plan of IAQ monitoring and spirometry tests. Confidence building among the occupants by highlighting that the outcome of the study would result in their future well-being. • The Questionnaire survey -Helps in identifying the community problems and makes all key decisions on set goals and objectives.
Objectives of present study • Community sensitization for existing inequality in IAQ • Quantification of IAQ i.e. indoor air pollutant monitoring in critical winter season • IAQ data Analysis i.e. IAQ inequality quantification • Effects of IAQ inequality - Respiratory health effects
Site Location Nizamuddin
Monitoring locations • Four houses were selected for the present study. • Three from low income group (LIG); and one from high income group (HIG).
Data • Indoor air pollutant(10 a.m. to 4 p.m. Monday, Wednesday and Friday, December, 2004 to February, 2005) RSPM i.e. PM10, PM2.5 and PM1.0 CO2 CO SO2 NO2 • Health Forced Vital Capacity (FVC) Forced Expiratory Volume in 1 sec(FEV1) • Survey Questionnaire consisting of household and respiratory health information
IAQ inequalities PM10, PM2.5 and PM1.0 concentrations, in both household types exceed the permissible limits.
IAQ inequalities • The CO2 concentration indoors exceeds the 1000 ppm due to inadequate ventilation during winters. • The concentrations of SO2, NO2, and CO are significantly low
IAQ inequalities -Consequences • 70% of the respondents suffering from cough, breathlessness and wheezing, 53.4% have cough and 16.6% have phlegm in urban poor households. • Among the urban rich, these symptoms are lower
IAQ inequalities -Consequences 50% of the occupants suffer from high level of respiratory problems among urban poor but only 20% among urban rich
IAQ inequalities -Consequences • Women are more vulnerable to respiratory problems than men. • Spirometry shows that severe obstructive ventilatory defects e.g. asthma were observed in urban poor households. • Urban rich households indicates lesser obstruction in the lung function
IAQ inequalities: Source and Cause Source-Wood stoves used for cooking Cause-Low household income.
IAQ inequalities: Source and Cause Source-Inadequate ventilation Cause-Lack of awareness
IAQ inequalities: Source and Cause Source Use of LPG for cooking Efficient ventilation Cause High household income Better standard of living Awareness
Conclusions 1)The concentrations of PM10, PM2.5 and PM1.0 are exceeding the permissible limits as prescribed in ASHRAE, 1989 in both households i.e. the urban poor and urban rich. 2) The use of woodstoves for cooking and inadequate ventilation are major sources & causes of high concentration of RSPM in urban poor and urban rich households, respectively. 3) In urban rich households, the use of cleaner fuels, smokecontrol appliances and location of cooking stoves reduce the concentrations of indoor air pollutants.
Conclusions • The respiratory problems such as cough, wheezing, breathlessness and phlegm are more prevalent in urban poor households than in urban rich. • The urban poor have a high score of respiratory problems indicating prevalence of respiratory diseases. 6) Women are more vulnerable to respiratory problems than men in both, urban rich and urban poor households. 7) The spirometry results (FEV1/FVC %) show severe respiratory obstructions among urban poor households.
Recommendations • Community participation in such monitoring produces cost-effective development of the data base. • Community participation effectively mobilizes the local support for necessary preventive and remedial measures. • Community participation is the only effective method to deal with IAQ inequalities among those societies where stratification in terms of money and living standards exist.
Thank You Mukesh Khare Atlantic LNG Chair Professor in Environmental Engineering, University of West Indies, St. Augustine, Trinidad and Tobago. E-mail: kharemukesh@yahoo.co.in Priyanka Kulshreshtha Research Scholar, Department of Civil Engineering, IIT Delhi, India. E-mail: pearlpriya@rediffmail.com