Download
1 / 25
270 likes | 620 Views
Ventilator Weaning with Spinal Cord Injury. & Tracheostomy. RISCI snapshot survey 2009. 18 patients in critical care beds awaiting transfer 5> 6 months. South of England Review of Standards in Spinal Cord injury. . National Spinal Cord Injury Strategy Board. .

E N D
Ventilator Weaning with Spinal Cord Injury & Tracheostomy
RISCI snapshot survey 2009 18 patients in critical care beds awaiting transfer 5> 6 months South of England Review of Standards in Spinal Cord injury National Spinal Cord Injury Strategy Board Weaning guidelines for Spinal Cord Injured patients in Critical Care Units
Ventilated spinal injured patients • 15-20% Initially ventilated • 98% Weanable • 1% Nocturnal ventilation • 1% Fully ventilator dependant • = 8-12 patients/yr • ~ 120 patients in UK
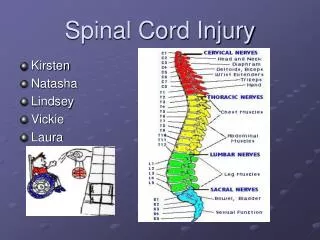
Respiratory effects Acute VC 1 Year VC Lumbar Unable to cough 100-70% 100-70% Low thoracic é chest wall compliance ê Vital capacity High thoracic éé chest wall compliance 30-50% êê Vital capacity poor expansion. Basal collapse 60-70% C5/C6 Diaphragms, Scalenes 20% 40-50% C3/C4/C5 Sternomastoid and partial diaphragm Above C3 Sternomastoid only 5-10%
Weaning Based on little evidence but vast experience Prerequisites Good pulmonary compliance Low FiO2 requirement Awake and cooperative Some respiratory activity Committed team
Any respiratory activity? Testing Volume measurement Beware sensitive ITU Vents Modified brainstem death test
Weaning Progressive ventilator free breathing Measure Vital Capacity VC Time off Vent <250 mls 5 Mins -500 mls 15 Mins -750 mls 30 Mins -1000 mls 60 Mins Measure VC Post weaning >70% pre weaning Southport Spinal Injury Centre Increase duration and/ or frequency
Weaning Wait for spasticity Bronchodilators ?High TV Ventilation (>20 ml/Kg)?1 Supine • The effect of tidal volumes on the time to wean persons with high tetraplegia from ventilators • Peterson W. et al spinal cord 1999 37(4):284-288
Weaning Off vent requires PEEP/CPAP to reduce atalectasis Best option cuff with speaking valve. Ditch the ITU vent Don’t reduce pressure support too far Try to stick to plan Aim for off all day, support at night
Speech essential Eating optional
How to wean BIPAP/ PS Slow weaners Fast weaners laryngeal function vs resp function VFB Cuff up Cuff down on vent VFB Cuff down speaking valve VFB speaking valve Downsized uncuffed tube Decannulate
How successful ? Southport spinal injuries unit • 246 patients over 20 years • 63% weaned • 33% Ventilator dependant • 4% Died
Post weaning Maintenance ‘ Maintain Range of Movements’ Manual hyperinflation IPPB Cough Assist/ Clearway Improve muscle strength Inspiratory muscle training
Tracheostomy • Surgical may be better than percutaneous • Safer if unstable spine • Anatomically accurate • Easier changes long term • Worse scar • Logistically difficult
Trachy Tubes Use what you are used to but… Avoid fenestrations
Trachy Tubes Definitely avoid
Trachy Tubes Definitely consider supraglottic suction tubes
Trachy Tubes If they need a tube long term
Trachy Tubes Don’t dismiss
Speaking valves Are not all the same
When to decanulate No respiratory support required Secretion clearance guaranteed