Download
1 / 24
730 likes | 2.59k Views
Acute Pain Management: Epidural Analgesia. Laura Yontz UNCC Nursing 6301 March, 2008 . Objectives. Describe the anatomy, physiology, pharmacology, and complications related to the analgesia techniques. Initiate nursing interventions to ensure optimal care. Recognize emergency situations.

E N D
Acute Pain Management: Epidural Analgesia Laura Yontz UNCC Nursing 6301 March, 2008
Objectives • Describe the anatomy, physiology, pharmacology, and complications related to the analgesia techniques. • Initiate nursing interventions to ensure optimal care. • Recognize emergency situations.
50% of patients report that their pain relief was inadequate. • Polomana, R (2008). Perspectives on pain management in the 21st century. Journal of Perianesthesia Nursing (23)1: 4-13.
Acute Pain Management Training Not a major portion of professional healthcare education
NC State Board of Nursing • Ongoing competence of nurses • Keep the public safe
Advisory Statement • Written protocol • Appropriate training • Supervised practice • Written approval within agency.
Epidural Analgesia • Low volume, high risk • How do you stay competent? • How do you provide safe care?
Epidural Analgesia • Success rate of 70% Viscusi, E. (2007) Emerging treatment modalities: Balancing efficacy and safety. Am J Health – Syst Pharm. 64: 6-10. • Catheters placed for procedures associated with significant pain • Krenzischek, D. (2008) Pharmacotherapy for acute pain: Implications for practice. JOPAN 23(1):28-42
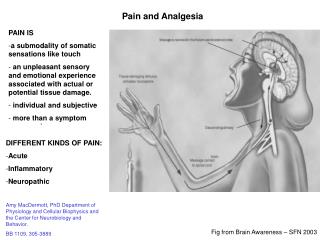
Anatomy • Epidural space • Contains; • Blood vessels • Fat • Nerves
Anatomy • Analgesics delivered through a needle into the epidural space • Catheter threaded into space
Method of Administration • Bolus • Continuous • PCEA
Characteristics of Epidural Drugs • Close to receptor sites. • Small doses effective • Cross dura mater into CSF, then into spinal cord to receptor sites.
Characteristics (cont.) Lipid soluble Water soluble • Fentanyl, sufentanil • Readily dissolve in epidural fat; move quickly into CSF, then into spinal tissue. • Rapid onset of action: 5 minutes • Shorter duration of action • Morphine, hydromophone • Do not traverse fatty dura mater as quickly • Once in CSF tend to stay there; eventually move into spinal tissue • Longer onset of action: 30-60 minutes • Longer duration of action
Local Anesthetics • Bupivicaine , ropivicaine • Used in combination with opioids • Moderate to fast acting: 5-20 minutes • Long duration of action: up to 12 hours • Work synergistically to provide better pain relief at lower doses
Side effects Pain management Nausea and vomiting • Vital signs • Pain behaviors • Analgesic history • Acceptable levels • Breakthrough pain • Common reaction • Treated with metoclopramide
Side effects (cont.) • Respiratory depression • RR less than 8 breaths/minute • Oxygen sat less than 90% • Decreased LOC
Side effects (cont.) • Urinary retention • Assess for distention • Foley catheter • Itching • Treated with benadryl
Side effects (cont.) Inadvertent IV infusion Rare side effects • Cardiotoxicity • Neurotoxicity • Abscess • Epidural hematoma • Caudal equina syndrome • Catheter migration • Sympathetic blockade • Allergic reaction • Local anesthetic toxicity
Nursing Responsibilities • Monitor vital signs • Assess level of sedation • Monitor side effects • Emergency equipment • Know your institution’s protocols
50% of patients report that their pain relief was inadequate. • Polomana, R (2008). Perspectives on pain management in the 21st century. Journal of Perianesthesia Nursing (23)1: 4-13.
Summary • Epidural analgesia safe and effective when monitored. • Patient receives stable, consistent pain relief. • Patient satisfaction increases. • Nurse responsible for providing safe, competent care for patients.
References • Kingsley, C.(2001). Epidural analgesia: Your role. RN 64(4): 9 • Krenzischek, D. (2008). Pharmacotherapy for acute pain: Implications for practice. JOPAN 23(1): s28-42. • Pasero, C. (2003). Epidural analgesia for postoperative pain. AJN 103(10): 62-64 • Pasero, C. (2003). Epidural analgesia for postoperative pain, part 2. AJN 103(11): 43-45
References (cont.) • http://www.ncbon.org/content Activities within the scope of practice for the RN/LPN (accessed online March 1, 2008.) • Polomano, C. (2008). Assessment, physiological monitoring, and consequences of inadequately treated acute pain. JOPAN 23(1): s15-27. • Viscusi, E. (2007). Emerging treatment modalities: Balancing efficacy and safety. Am J Health-Syst Pharm. Vol 64, March 15, 2007 suppl 4 (accessed online March 1, 2008 via Cinahl).