Download
1 / 65
800 likes | 1.72k Views
Fungal Infections of the Skin and Nails. Adam O. Goldstein, MD, MPH Associate Professor Department of Family Medicine University of North Carolina at Chapel Hill aog@med.unc.edu. Fungal Infections of the Skin and Nails. Objectives

E N D
Fungal Infections of the Skin and Nails Adam O. Goldstein, MD, MPH Associate Professor Department of Family Medicine University of North Carolina at Chapel Hill aog@med.unc.edu
Fungal Infections of the Skin and Nails Objectives 1. To distinguish common fungal infections from similar appearing lesions; e.g. eczema 2. Improved dx of fungal lesions with a KOH scraping 3. Know at least 2 tx options for common fungal infections of the skin & nails 4. Know common errors in fungal dx and tx 5. Know when to suspect & how to dx ID reaction
Superficial Fungal Infections • 4.1 million visits -82% nondermatologists • 3 types of fungi-dermatophytes: Epidermophyton Trichophyton Microsporum • Named by location • Similar treatments; Varied presentations
Superficial Fungal Infections • Common Denominator = Do KOH, Do KOH, Do KOH .. • Nondermatologists (34%) were more likely than dermatologists (5%) to prescribe combination products for the treatment of common fungal skin infections; savings = $10-25 million. (Smith, JAAD,1998)
ID Reaction • Severe inflammatory skin reaction • Immunologically mediated • Appearance may be very different from original lesion • Fungal infections if severe enough may provoke ID reaction. If you do not think about it, you will not diagnose it.
Tinea capitis • Trichophyton or Microsporum species • Disease of children • Exposure from other children or pets • Highly variable presentation
T. capitis • Primary lesions: plaques, papules, pustules or nodules • Secondary lesions: scale, alopecia, erythema, exudate and edema Kerion: Severe T. capitis- inflamed, boggy nodule with hair loss
T. capitis Diagnosis • Overdiagnosed in adults, underdiagnosed in children • Direct microscopic exam of hairs looking for hyphae/spores • Woods lamp: bright green fluorescence in hair shafts d/t Microsporum infection (< 20% time) • Culture: If KOH is negative but strong clinical suspicion
T. capitis Differential Diagnosis • Seborrheic dermatitis- rare in children, KOH - • Cellulitis- may coexist, KOH - • Alopecia areata-discrete, nonscaling areas hair loss • Syphilis- “mothball eaten” areas
T. capitis Treatment • Systemic therapy needed • Griseofulvin at least 8 wks (Or 2 wks beyond cure) • Itraconazole- 3-5mg/kg/day 1x/week 3 weeks • Fluconazole- 3-6 mg/kg children (10, 40 ml) • Terbinafine - 3-6mg/kg/day X 4 weeks
Griseofulvin • Microsize 250, 500 mg tabs, 125 mg/5 cc susp • 500-1000 mg/day adults • 15-20 mg/kg/day children • SE’s: photosensitivity, H/A, GI upset, hypersensitivity, leukopenia • Active only against dermatophytes, not yeasts
T. capitis Patient education • Compliance for 2 weeks beyond “cure” to prevent relapse • Look for sources of infections • Clean contaminated objects • Reassure caretakers that it may take 1 month for improvement
Tinea barbae Characteristics • Inflammation in the beard/hair • Pseudofolliculitis • Frequently “failed” antibiotics • Positive S.Aureus culture does not rule out T. barbae
T. barbae Diagnosis • Nodular, boggy lesions with exudate • Sinus tract formation • Scarring if untreated • KOH or culture may confirm
T. barbae Differential diagnosis • Bacterial folliculitis • Pseudofolliculitis barbae • Contact dermatitis • Herpes • Syphilis • Acne • Candida
T. barbae Treatment • Griseofulvin 0.5-1 g/day • Itraconazole or terbinafine for resistant cases • Local care
Tinea corporis • Papules or plaques with erythema and scale • Look for annular lesions with central clearing • Well-demarcated edges
T. corporis Diagnosis • KOH from leading edge • Prior steroid use alters response/appearance • Majocchi’s granuloma: pluck hairs for hyphae
T. corporis Differential diagnosis • Nummular eczema KOH neg • Pityriasis rosea KOH neg, multiple papules/plaques • Psoriasis KOH neg, thick, silvery scales • Granuloma annulare KOH neg, no scale • Lyme disease KOH neg, no scale
The diagnosis please... Lichen simplex chronicus Nummular eczema
T. corporis Treatment • Avoid “Lotrisone” type combos • Topical agents for mild/moderate disease • Oral agents for extensive/resistant disease • Continue topical medication 7-14 days beyond “cure”
Tinea cruris • Thrives in humid environments • Diagnosis: • Spares scrotum; • Pruritus & burning clues • Look for feet as possible infection source • KOH + hyphae
T.cruris Differential Diagnosis: • Candida Beefy red with poorly defined borders • Intertrigo KOH negative, irritant dermatitis • Erythrasma Asymmetric velvety patches, Neg KOH • Psoriasis Thick silvery scales,Neg KOH • Seb derm Borders less defined, distribution different, Neg KOH
T. cruris Treatment • Topical agents for 2-3 weeks • Mild topical steroid for inflammatory component • Pruritus relief • Look for infection source
T. cruris Patient education • Use topical meds 7-14 days beyond cure • Avoid prolonged topical steroids • Avoid self-medicating preps • Avoid baths and tight fitting underwear • Use mild soaps or soap substitute • Antifungal powders • Keep area dry
Tinea manus • Diagnosis: • Often unilateral, but with bilateral feet • May have only scant scaling, vesicles • Differential Diagnosis: Eczema, contact dermatitis • Treatment: Topical agents
Tinea pedis • Diagnosis: • Extremely variable presentation • Be aware of id reaction and bacterial infection
T. pedis • Differential Diagnosis: • Eczema, Contact, Psoriasis, Keratolysis • Treatment and Patient Education: • Limited: Antifungal creams X 1-4 weeks; • Severe: Oral therapy • Griseofulvin 500 mg microsize bid X 4-8 weeks • Terbinafine 250 mg/day X 2-6 weeks
Tinea Versicolor • Diagnosis: macules, plaques; fine scale after scraping; KOH +
Tinea Versicolor • Treatment: Limited disease: Topical agents Widespread: Ketoconazole 200 mg X 2 one dose, repeat 1 week (Not griseofulvin) • Prevention and Patient Education: Selenium sulfide 2.5% overnight 1X/month
Candidiasis • Diagnosis: Beefy red lesions, satellite papules and pustules • Differential Dx: Tinea, Intertrigo • Treatment and Patient education : Topical antifungal creams Oral therapy for extensive (not Griseofulvin) Environmental: Zeasorb powder or Burow’s Mild topical steroids
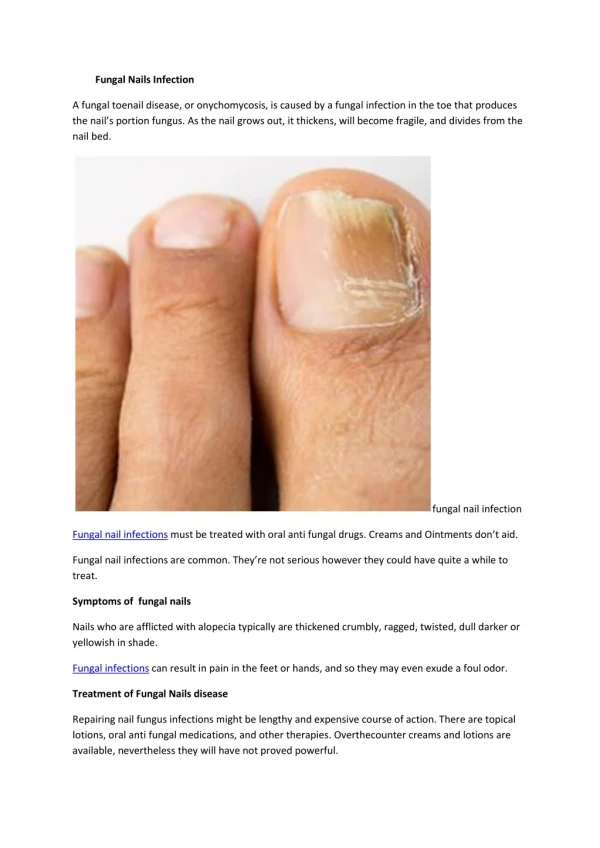
Onychomycosis • Why should we treat? (cosmetically disfiguring, painful, entry for cellulitis) • Diff Dx: Psoriasis, Lichen Planus, Trauma • Diagnosing vs. treating
Diagnosis? • Culture? • Treatment?