Download
1 / 13
130 likes | 255 Views
Learning To Make a Difference. VTE Assessments in Acute General Medicine at the John Radcliffe Hospital. Srimathy Vijayan CMT 1, John Radcliffe Hospital. Rationale. Encompassed in the NICE VTE guidelines (Jan 2010) Important issue:

E N D
Learning To Make a Difference VTE Assessments in Acute General Medicine at the John Radcliffe Hospital Srimathy Vijayan CMT 1, John Radcliffe Hospital
Rationale • Encompassed in the NICE VTE guidelines (Jan 2010) • Important issue: • Patient Safety - VTE prophylaxis shown to reduce the number of deaths in patients • Trusts are monitored re. performance and financial implications are great
Project Aim(s) • By July 2012, 100% of patients admitted via AGM will have VTE assessments completed within 24 hours of admission • To ensure that in 100% of cases of those NOT on VTE prophylaxis, there is clear documentation as to why in the medical notes and a corresponding online VTE assessment completed
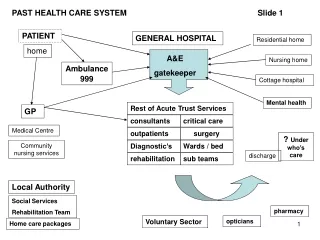
Process mapping Daily RV for need of VTE prophylaxis Pt admitted to AGM Appropriate prescription of VTE Seen by Dr : History, Examination, Investigations, Diagnosis considered Online completion of VTE assessment form Management Plan: including need for VTE
Driver Diagram VTE assessments in AGM Education on Drs part Access to case notes Prescribing correctly in DC Review by Seniors Integral part of pt admission like DC/CXR etc… Reasons for VTE and NOT for VTE Locums who do not have this must inform others Appropriate dosing as per protocol Review on PTWR using appropriate proforma
Methods • Performed at JR Hospital, Level 7 (AGM wards), 3 Wards selected • 5 patients on each ward randomly selected. For each patient: • Admission date noted • Drug chart screened for VTE prescription • For those who did NOT have VTE prescribed Medical notes screened for explanation • Online system ‘casenotes’ used to determine whether VTE assessment was completed and on what date • Those Pts not on VTE – online case notes assessment evaluated to see if it corresponds with NOT needing VTE
Methods contd… • Data Collection: • Baseline (Week 0), Week 1, Week 2, Week 3 • Intervention: • 1 day after Baseline data collected • Consisted of Email to all Staff working on AGM
Results Number of Patients who were not on VTE and percentage of those with reasons for no VTE
Results Number of Patient who were not on VTE and had correctly completed online VTE assessments
Discussion • By Week 3, Target of 100% for VTE assessments completed within 24 hours of admission achieved. • Ongoing Issues with ‘poor documentation’ as to why patients are not on LMWH - why? • For those patients not on VTE – the online form very rarely reflects ‘no VTE required’ or ‘offer anti-embolic stockings’ only. In the Majority of cases still filled out as needing prophylactic VTE – why?
Next Steps • What do you plan to do next? • Continue data collection for a few further weeks to evaluate trends • Discuss results with local Audit department • Address the issues of poor documentation in notes for those not on VTE – perhaps at next AGM clinical governance meeting? As well as need for accurate VTE completion online and ‘updating’ issue • What has been the learning? • The importance of the need to consider VTE in pts admitted to hospital and the need to document in those cases where you feel VTE not appropriate