Download
1 / 39
390 likes | 598 Views
DEBATE: Do we have enough data to eliminate chemotherapy from initial CLL therapy? Can kinase inhibitors and IMiDs replace chemotherapy? Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute October 25, 2013. Previously Untreated CLL. Purine nucleosides

E N D
DEBATE: Do we have enough data to eliminate chemotherapy from initial CLL therapy? Can kinase inhibitors and IMiDs replace chemotherapy? Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute October 25, 2013
Previously Untreated CLL • Purine nucleosides • - Fludarabine • - Pentostatin • - Cladribine Purine nucleosides and alkylators 30% CR Better PFS 5% - 20% CR Better PFS in younger pts Chemo-immunotherapy (CIT) 45% CR; better PFS & OS Alemtuzumab monotherapy 24% CR Bendamustine 30% CR 1960s 1970s 1980s 1990s 2000s • Alkylating agents • - Chlorambucil • - Cyclophosphamide 5% CR
CLL8: Progression-Free Survival Median PFS: FCR: 51.8 mo FC: 32.8 mo (N=790 Hazard ratio 0.563, p<0.001) PFS rate 3 yrs post randomization: FCR: 64.9% FC: 44.7% P<0.001
Incidence of Refractory Disease 20-35% to single agent fludarabine In GCLLSG CLL8: 30.9% of patients progressed within two years
CLL: Problems with Chemotherapy Continuous relapse at progressively shorter intervals and progressive resistance to therapy Patients with 17p and/or complex cytogenetics respond poorly from the start Elderly patients (most!) tolerate chemotherapy poorly Myelosuppression, often persistent Risk of tMDS / AML Immunosuppression, often persistent Increased infection risks ? Increased risk of second malignancies Clonal evolution: ? Selection for pre-existing adverse clones vs induction of new clones
What are the Alternatives? Mature data in previously untreated patients: (+/- rituximab) Lenalidomide Idelalisib (GS1101, CAL101) Ibrutinib Evolving data: Obinutuzumab Highly effective novel agents not yet tested upfront: IPI-145, ABT199
What about Lenalidomide? Immunomodulatory agent Promotes CLL cell activation but is not cytotoxic Promotes T cell function Effective in relapsed refractory CLL with ORR 35-50% BUT can be difficult to tolerate, with tumor flare, tumor lysis, myelosuppression Often better tolerated with antibody given first Mechanism of action still unclear
Lenalidomide for Upfront Therapy in Elderly CLL Patients 88% 60% Median F/U 24 mos Blood 2011; 118:3489
Lenalidomide for Upfront Therapy in Elderly CLL Patients At 4 yr follow-up: TTF NR OS 82% N=35 (58%) had DOR >36 mos: 71% CRs 29% PRs Blood 2013; 122:734
Immune Parameters Improved on Lenalidomide T cells Immunoglobulins
Lenalidomide: Best Response (n=25) Median time to best response 18.1 months (1.8-63.4) Chen C, et al: ASH 2012
PFS and OS Outcomes (n=25) • 7 patients have progressed • 2 developed Richter’s transformation after discontinuation, 2 skin cancer, 1 recurrence of remote lung cancer 3 year PFS 64.6% (95% CI: 47.5-87.8%) 3 year OS 85.3% (95% CI: 71.1-100%)
Summary: Status of Lenalidomide Mature data in previously untreated elderly patients looks very promising BUT pivotal phase 3 study LEN vschlorambucil closed early due to excess of deaths on LEN arm, plus many patients dropped out early on that arm Especially in patients >80
Targeting Kinases in the BCR Pathway Idelalisib(GS-1101; CAL-101) Ibrutinib (PCI-32765)
Idelalisib: Highly Selective for PI3K Delta 100 Basophil Activation FceR1 75 % +CD63 Cells EC50=65 nM Whole Blood (normalized(control) 50 PMBC (n=9) Whole Blood (n=20) 25 0 0.0001 0.001 0.01 0.1 1 10 100 CAL-101 ( M) m Less than 10-fold shift in EC50 in whole blood
Phase 2 Single Arm, Open Label Study Study Schema Extension Study: 101-99 Primary Study: 101-08 Subject Accrual Oct 2010 Through Apr 2012 • Therapy continues as long aspatient receives benefit • Idelalisib (150 mg BID) x 48 wks • Rituximab • (375 mg/m2) • weekly x 8
Idelalisib + R Nodal Response at 8 Weeks Best Nodal Response • Not evaluable N = 14 • Patients without adenopathy at baseline, N = 12 • Early withdrawal, N = 2 • Not evaluable N = 16 • Patients without adenopathy at baseline, N = 12 • Early withdrawal, N = 2 • No assessment, N = 2 * Assessed by Physical Exam or CT
Response Assessment • Median Time to Response 1.9 months • 24/26 patients with B symptoms resolved by week 16 No on-study progression
Improvement in Cytopenias • Hematologic response rate • 17/17 with Anemia • 16/17 with Thrombocytopenia • 5/5 with Neutropenia
All Cause AEs ≥25% in Primary and Extension Studies; On-Study Lab Abnormalities
Progression-Free Survival PFS at 24 months: 93% *ITT analysis of primary + extension study Extension study assessments based on standard of care
Ibrutinib (PCI-32765): BTK Inhibitor Forms a specific and irreversible bond with cysteine-481 in Btk Potent Btk inhibition IC50 = 0.5 nM Orally available Once daily dosing results in 24-hr sustained target inhibition O N H 2 N N N N N O
PCYC-1102-CA: Phase Ib/II in CLL/SLL (Treatment Naïve ≥ 65 yrs population) *The 840mg TN cohort was terminated after comparable activity and safety between doses was shown in R/R patients. One patient in this cohort received only 420 mg daily.
PCYC-1102-CA: Patient Disposition(Treatment Naïve ≥ 65 yrs) # days on ibrutinib: a) 280 days; b) 41 days; c) 115 days; d) 41 days; e) 9 days
Common AEs (>20%) Regardless of Relationship Grade 1 Grade 3 Grade 2 Grade 4
SafetyAdverse Events ≥ Grade 3 Hematologic Infectious Grade 3 Grade 4 Grade 5
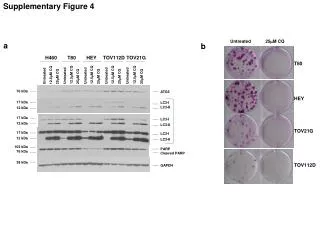
Best Response 71% 3/31 13% 4/31 CR PR PR w/ lymphocytosis 58% 18/31 SD PD 13% 10% 4/31 3/31 Treatment Naïve(n=31) 2 not evaluable
PCYC 1102: Best Overall Response by Risk Features aOverall response rate and 95% exact binomial CI
Durable Remissions with Ibrutinib Monotherapy as Initial CLL Therapy
Summary Mature follow-up data with lenalidomide, idelalisib-R, and ibrutinib demonstrate at least comparable and possibly improved PFS vschemoimmunotherapy Oral agents are preferred by patients and toxicities are manageable Can we improve further on these outcomes?
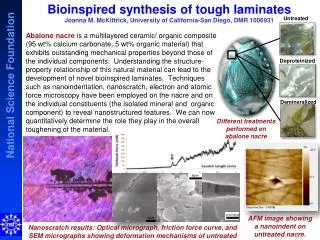
GA101: Mechanisms of Action Enhanced ADCC Glycoengineering forincreased affinity to FcγRIIIa Increased Direct Cell Death Type II versus Type I antibody Effectorcell B cell Lower CDC Type II versus Type I antibody Complement GA101 FcγRIIIa CD20
GA101: 1,000 mg days 1, 8, and 15 cycle 1; day 1 cycles 2–6, every 28 days Rituximab: 375 mg/m2 day 1 cycle 1, 500 mg/m2 day 1 cycles 2–6, every 28 days Clb: 0.5 mg/kg day 1 and day 15 cycle 1–6, every 28 days Patients with progressive disease in the Clb arm were allowed to cross over to G-Clb CLL11: Study Design Additional 190 patients to complete stage II Stage I, n = 590 RANDOMIZE 1:2:2 Chlorambucil x 6 cycles Previously untreated CLL with comorbidities Total CIRS* score > 6 and/or creatinine clearance < 70 ml/min Age ≥ 18 years N = 780 (planned) Stage IaG-Clb vs Clb Stage IbR-Clb vs Clb GA101 + chlorambucil x 6 cycles Stage IIG-Clb vs R-Clb Rituximab + chlorambucil x 6 cycles *Cumulative Illness Rating Scale
Summary Kinase inhibitors and IMiDs (+/- anti-CD20 antibody) show durable remissions in previously untreated patients Randomized comparisons to CIT ongoing ECOG FCR vs IR age < 70 Alliance BR vs IR vs I age 65+ Additional drugs (IPI-145, ABT199) are poised to add to this landscape How do we best combine these agents, i.e. how much does the antibody add? Is rapid remission induction important?
Open Questions How durable are the remissions in 17p patients? How do we best sequence different novel agents? Are more relapses occurring as Richter’s transformation, even in previously untreated patients? What are the long-term side effects of continued therapy? Where do SCT or CAR T cell therapy fit?
Previously Untreated CLL • Purine nucleosides • - Fludarabine • - Pentostatin • - Cladribine Purine nucleosides and alkylators 30% CR Better PFS 5% - 20% CR Better PFS in younger pts Chemo-immunotherapy (CIT) 45% CR; better PFS & OS Alemtuzumab monotherapy 24% CR Bendamustine 30% CR 2010s 1960s 1970s 1980s 1990s 2000s • Alkylating agents • - Chlorambucil • - Cyclophosphamide Novel Targeted Therapies (BCR, BCL2, IMiDs, ?) + Monoclonal Antibodies 5% CR
Acknowledgments RichardFurman, Susan O’Brien, John Byrd, John Seymour, ValentinGoede Brown Lab, DFCI Bethany Tesar Stacey Fernandes Sasha Vartanov Reina Improgo Josephine Klitgaard Clinical Research Karen Francoeur Caitlin Tesmer-Brier Karen Campbell Shannon Milillo Hazel Reynolds Broad Institute Eric Lander Gaddy Getz Carrie Sougnez NirHacohen Stacey Gabriel Mike Lawrence PetarStojanov AndreySivachenko KristianCibulskis David Deluca Wu Lab, DFCI Catherine Wu Dan-Avi Landau LiliWang YouzhongWan Lymphoma Program, DFCI Arnold S Freedman David C Fisher Ann S LaCasce Eric Jacobsen Philippe Armand Matthew Davids Okonow-Lipton Fund Melton Fund Rosenbach Fund Center for Cancer Genome Discovery, DFCI Megan Hanna Laura Macconaill NIH, NHGRI CLL Research Consortium DFCI Biostatistics Donna Neuberg Lillian Werner Haesook Kim Kristen Stevenson