Download
1 / 42
1.11k likes | 5.18k Views
VARICOSE VEINS. DR. RYAN FERNANDES MODERATOR:- DR.ASHOK HEGDE AJIMS. ANATOMY. Dilated, tortuous and elongated superficial veins of the lower limb are called varicose veins. Veins are specifically designed to allow flow in one direction. Presence of numerous valves prevent venous reflux.

E N D
VARICOSE VEINS DR. RYAN FERNANDES MODERATOR:- DR.ASHOK HEGDE AJIMS
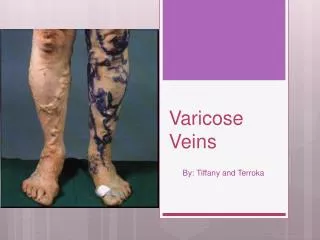
ANATOMY • Dilated, tortuous and elongated superficial veins of the lower limb are called varicose veins. • Veins are specifically designed to allow flow in one direction. • Presence of numerous valves prevent venous reflux.
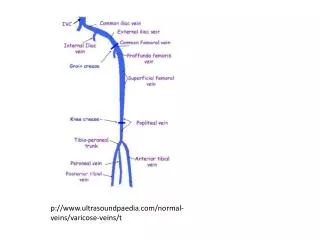
The veins of the lower limbs are divided into 3 grps-: • Deep veins • Superficial veins • Communicating/ perforating veins.
Superficial veins- act as conduit taking blood from surface to deep veins via perforating veins. • Long saphenous vein- orginates in the medial border of the foot from tributaries of the dorsl venous arch, ascends in front of medial malleolus and run along the medial side of the leg. • Accompanied by saphenous nerve below the knee.
Anterior and posterior branches joined the LSV below the level of knee. • At the level of knee LSV lies superficially in posterior position.in the thigh LSV passes antero superiorly up the medial side of thigh to reach the saphenous opening in deep fascia to join the femoral vein. • Tributaries near its termination- superficial cicumflex illiac, sup epigastric, sup external pudendal.
Short saphenous vein-arises at the lateral border of the foot and passes upward behind the lateral malleolus and lies over the lat and the post aspect of the leg and enters the deep fascia in the popliteal fossa to join the popliteal vein.
Deep veins- tibial , popliteal, femoral veins are the deep veins which drain blood into the illiac veins and than to IVC. • Pumping veins are venous sinuses in calf muscles which pumps blood towards major veins, also called as musculo-venous pumps.
Perforating veins- They connect sup to deep veins at various levels, guarded by valves • - ankle perforators(may or kuster) • - lower leg perforators(1,2,3) cockett • - below knee perforator(boyd) • - mid thigh perforators (dodd)
PHYSIOLOGY • Lower limb veins allow flow from distal to proximal and from superficial to deep , but prevent retrograde flow. • Venous valves are abundant in distal lower limb. • Arterial pressure across the capillary increases the pumping action of vein. • Calf muscle pump-alternate contraction and relaxation of the muscles of the leg. • Negative intrathorasic pressure.
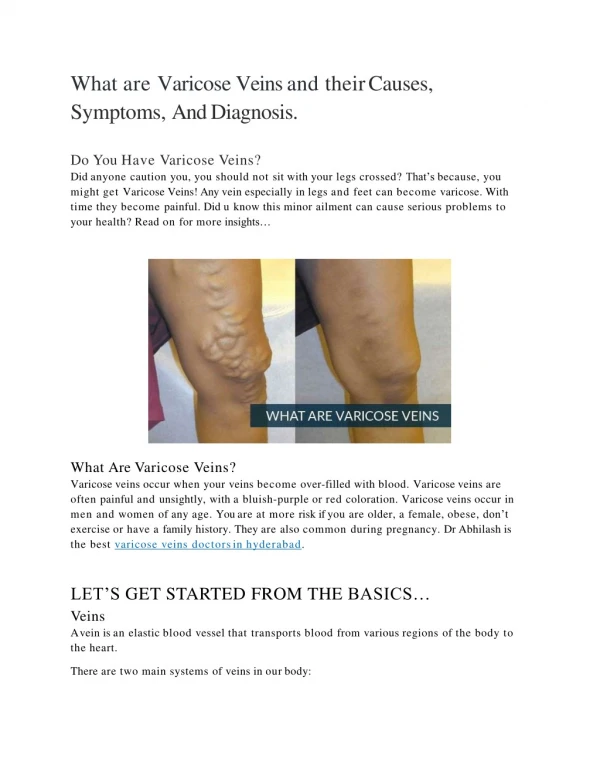
Varicose Veins Valve (open) Skeletal muscle Valve (closed) Venous valves Vein Direction of blood flow
TYPES • Long saphenous vein varicosity • Short saphenous vein varicoisity • Varicose vein due to perforator incompetence • Thread veins • Reticular varices
Etiology • Primary varicosity • Congenital incompetence or absence of valves • Weakness or wasting of muscles • Stretching of deep fascia • Klippel – Trennuaney syndrome, familial • Secondary varicosity • Recurrent thromboplebitis • Pregnancy • Pelvic tumors • OCP’s • Occupational • Obstruction to venous return eg: abdominal tumors • Retroperitoneal fibrosis • AV malformation • Iliac vein thrombosis
Other sites • Esophageal varices • Hemmorhoids • Varicocele • Vulva • Caput medusa
Pathogenesis -Venous Diseases • Two theories • Fibrin cuff theory • White cell trapping theory
Incompetence of venous valves • Stasis of blood • Chronic venous hypertension • Defective microcirculation • RBC diffuses into tissue planes • Lysis of RBC’s
Release of hemosiderin • Pigmentation • Dermatitis • Capillary endothelial damage • Severe anoxia • Chronic venous ulceration
Inappropriate activation of trapped leucocytes release proteolytic enzymes which cause cell destruction and ulceration- white cell theory • Fibrin deposition. Tissue death, scaring occur together called as lipodermatosclerosis
Classification of lower extremity venous disease • C- clinical signs (0-6) • E- etiology (congenital, primary, secondary) • A- anatomy ( superficial, deep, perforator, or combination) • P- pathophysiology ( reflux, obstruction or both)
Clinical classification • 0- no visible signs • 1- telangectasia, reticular veins, flare • 2- varicose veins • 3- edema without skin changes • 4- skin changes due to venous diseases • 5- skin changes with healed ulcer • 6- skin changes with active ulcer
Clinical features • More common in females • Visible dialted veins in the leg with dragging pain and nocturnal cramps and feeling of heaviness • Pigmentation, Ulceration, eczema, dermatitis, bleeding • Pedal edema • Restricted ankle movements • Skin thickening
Signs • Trendelenburg test • Type 1 • Type 2 • Schwartz test • Multiple torniquet test • Fegans test • Modified perthes test • Morriseys cough impulse test
Complications of varicose veins • Haemorrhage • Eczema and dermatitis • Venous ulcer • Marjolin Ulcer • DVT • Lipodermatosclerosis • Equino varus deformity • Calcification • Thrombophlebitis
Investigations • Venous doppler • Duplex scan • Venography • Plethysmography • Ultrasound abdomen
Duplex Ultrasonography Superficial and deep systems evaluated Physiologic reflux: < 0.5 sec Pathologic reflux: > 0.5 sec
Treatment • Conservative • Injection line of treatment • Surgical • Newer Methods
Conservative • Crepe bandage • Unna boots • Limb elevation • Pneumatic compression method • Medical • Calcium dobesilate 500mg BD • Diosmin 450mg BD
Injection line of treatment • Indication of Sclerotherapy • – Uncomplicated perforator incompetance • - Smaller varices • - Recurrent varices • - Isolated varicosities
Sclerosant used – Sodium tetradecyl sulphate 3%, hypertonic saline , polidocanol • MOA – Causes aseptic inflammation, cause approximation of the intima leading to obliteration by endothelial damage • Other techniques of sclerotherapy - Microsclerotherapy - Trans illumination microsclerotherapy - Foam sclerotherapy - ECHO sclerotherapy
Contraindications of sclerotherapy - SF incompetance - DVT - Huge varicosities • Advantages - OPD procedure - No requirement of anaesthesia • Disadvantage - Anaphylaxis ,hyperpigmentation
Trendelenburg operation – Juxtafemoral flush ligation where saphaneous vein is ligated at SF Junction and LSV stripping is done. Stripping of vein – Using Myer’s strippers, - Complications – Injuries to saphaneous nerve. - Stripping is not done usually for veins in the lower part of leg in LSV Surgical
Ligation of the SSV at sapheno popliteal junction Stab Avulsion Technique Subfascial ligation of Cockett & Dodd Subfascial endoscopic perforator surgery
Newer methods Radiofrequency ablation (VNUS closure method) Trivex method Endovenous laser ablation (EVLA)
VARICOSE VEIN – EVLA (Endovenous Laser Ablation) • Patient Suitability Reasonably straight veins Recurrent Varicose veins following ligation alone • Mechanism of Action Heat generated by laser produces steam bubbles that cause thermal damage to endothelium and sub endothelial layer resulting in focal coagulative necrosis and shrinkage leading to thrombotic occlusion of the vein
ENDOVENOUS LASER ABLATION ( EVLA ) DIODE LASER 1 3 2
ADVANTAGES Day Care procedure Avoids GA No Scars Rapid Recovery
Complications of surgery - Infection - DVT - Haematoma formation - Nerve injuries - Recurrence