Download

1 / 40
490 likes | 1.5k Views
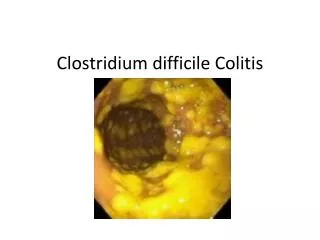
Clostridium Difficile. Stratification and Treatment Patient Case Robert Thompson PharmD Candidate Intermountain Medical Center August 9, 2013 . Learning objectives. Describe the roll of good intestinal flora Identify the epidemiology and pathophysiology of Clostridium difficile

E N D
Clostridium Difficile Stratification and Treatment Patient Case Robert Thompson PharmD Candidate Intermountain Medical Center August 9, 2013
Learning objectives • Describe the roll of good intestinal flora • Identify the epidemiology and pathophysiology of Clostridiumdifficile • Recognize the risk factors for infection • Stratify the different categories of Clostridiumdifficile • Establish a treatment regimen for a patient with Clostridiumdifficile
History of present illness • Louis Bowel (LB) is a 64 yo male admitted for epistaxis on 6/19/13 with a life threatening bleed, later diagnosed with a stroke • He is discharged to the rehabilitation floor on 6/21/13 to undergo therapy • Upon transfer to rehabilitation he has diarrhea and severe abdominal pain
Past medical history • COPD • H/O recurring epistaxis episodes since 2006 • HTN • H/O falls resulting in rib fractures • BPH • Recent sinus infection positive for S. pneumonia
Labs : 6/19/13 134 102 9 107 3.7 21 0.46 C. diff 9.2 253 9.6 28.1
Physical exam: 6/21/13 • Vitals: • BP – 167/106 • RR – 34 • Sat. Ox – 97% on O2 • Abdomen • Soft, non-tender • Active bowel sounds • HR - 112 • Temp – 36.4˚
Physical exam: 6/21/13 • Extremities: • 1+ RLE edema • Lungs: • Volume out is greater than volume in on both sides • Wheezing on exhale
Social history • Alcohol abuse (750 ml/day of vodka) • 2 pack/year smoker (decreased in the last year) • Divorced, lives in an apartment alone His daughter lives in the same complex and will be able to assist in his care
Medications • No home medications were reported • Medications at time of transfer: • albuterol/ipratropium neb 4 times daily • multivitamin 1 tablet VFTdaily • pantoprazole 40 mg IV daily • vit. D3 2000 units VFTdaily • heparin 5000 units SQ tid • flonase 2 sprays each nostril daily • chlorhexadine 15 ml swish and suction tid
Medications • Before admission to the rehabilitation unit, LB was given imipenem X 7 days for a sinus infection. The exact dose and route of imipenem was not available • He was started on vancomycin 1000mg IV Q12h on 6/18/13 which was changed to Q8h on day 2 and then d/c on day 3 • On 6/22/13, LB was started on amoxicillin/clavulanate VFT bid X 15 days for unresolved sinusitis
The human digestive tract is home to more than 500 species of microorganisms. Flipper.diff.org
Intestinal Flora • When healthy, this colonization is not only beneficial, but necessary to the host • Normal flora helps with digestion and absorption of nutrients as well as enhanced immunity from infectious agents 2013. www.cdc.gov/HAI/cdiff
www.equiotic.com • Normal flora protect the intestinal wall from pathogenic bacteria
Probiotics • Probiotics aren’t regulated by the FDA • Inconsistencies in products makes significant data hard to acquire • Meta-analysis showed benefit in C. diff prophylaxis. However, there were substantial data sets missing, so it is difficult to make a definitive conclusion as to how helpful this treatment would be • IDSA guidelines do not recommend using probiotics for C. difficile prophylaxis Goldenburg JZ, et al. Cochrane. 2013; 5. Cohen, S, et al. 2010 Shea-IDSA.
Epidemiology • The incidence of Clostridium difficile Associated Diarrhea (CDAD) increased 2 fold from 1996 – 2003 (61 in 100,000) • Rates increased 10 fold in patients over the age of 65 (43 in 1,000) • New strains such as NAP1/BI/027 are more virulent and have higher resistance than their ancestors Lamont J, et al. UpToDate2013 Jul 30
Epidemiology • CDAD is more likely with new exposure, while previously exposed individuals are more likely to not develop symptoms • Clindamycin used to be known as the most likely antibiotic to cause C. difficile • Fluoroquinolones are emerging as the new perpetrator. The NAP1/BI/027 appears to be correlated to fluoroquinolone use Lamont J, et al. UpToDate2013 Jul 30
Risk factors • Antibiotic use • Hospitalization or long term care facility • Health care workers • Advanced age (>64) • Suppression of stomach acid (PPI)? • Chemotherapy • Gastrointestinal tract manipulation (including tube feeds) Cohen, S, et al. 2010 Shea-IDSA
Proton Pump Inhibitor (PPI) • In a 2011 study, it was determined that PPI use increases a patients risk for C. diff 2 fold • The study couldn’t show causation but in the meta-analysis that looked at 30 studies and over 200,000 patients, there was a strong correlation between PPI use and C. diff Deshpande A, et al. Clinical Gastroenterology and Hepatology; 10(3). P 225-33
Patient case Which risk factors does LB have? • Recent antibiotic use • Long hospital stay • Tube feed • PPI use • Age? (64)
Pathophysiology • Colonization is facilitated through oral-fecal route • C. difficile releases two protein chain toxins: toxin A and toxin B • When these toxins gain intracellular entrance, they inhibit Rho protein facilitated regulatory pathways and lead to cell apoptosis Cohen, S, et al. 2010 Shea-IDSA
Pathophysiology • Toxin A stimulates inflammation and initiates intestinal fluid secretion • Toxin B is responsible for the virulence of C. difficille and strains that lack toxin B will colonize without being pathogenic Cohen, S, et al. 2010 Shea-IDSA
Stratification Cohen, S, et al. 2010 Shea-IDSA
Treatment • Initial episode (mild to moderate) • Metronidazole 500 mg PO tid X 10 – 14 days • Initial episode (severe) • Vancomycin 125 mg PO four times daily X 10 – 14 days • Initial episode (severe complicated) • Vancomycin 500 mg PO (or NGFT) four times daily + metronidazole 500 mg IV Q8h Cohen, S, et al. 2010 Shea-IDSA
Treatment • First recurrence • Same treatment as initial episode • Second recurrence • Vancomycin in a tapered and/or pulsed regimen Cohen, S, et al. 2010 Shea-IDSA
New options • Fidaxomicin (Dificid®) • Macrolide that is minimally absorbed so there are minimal side effects • Dosed at 200 mg PO bid X 10 days • Very expensive ~ $270/day • Similar efficacy to vancomycin, but less recurrence • Not tested against metronidazole Louie T, et al. NEJM. 2011
Fidaxomicin • In a multi-center, randomized, double blind, non-inferiority trial, fidaxomicin 200 mg PO bid was compared to vancomycin 125 mg PO 4 times daily both for 10 days for treatment of C.diff • It was evaluated on both per-protocol and intention-to-treat populations. In both analyses fidaxomicin was found to not be inferior to vancomycin • Fidaxomicin was also found to have less recurrence Louie T, et al. NEJM. 2011
Fidaxomicin • Where is it’s place in therapy? • When the guidelines were published, fidaxomicin was not on the market • It has proven to be as effective as vancomycin, but the cost difference is drastic ($355/day for fidaxomycinvs$124.50/day for vancomycin) Louie T, et al. NEJM. 2011 Red Book, 2013.
Patient Case • LB was tested again for C. diff after being admitted to rehabilitation and tested positive on 6/21/13
Patient case Looking at LB’s labs, what is the proper classification for his disease?
Patient case • LB was initiated on metronidazole 500 mg PO tid for 14 days on 6/22/13 Was this the appropriate regimen? Why?
Patient case • LB’s diarrhea and abdominal cramping persisted despite treatment. His labs were redrawn on 7/7/13. He was found to still be C. diff positive What is LB’s level of severity now? 9.6 4.2 283 29.5 SCr = 0.42
Patient Case • Metronidazole? • Vancomycin? • Fidaxomicin?
Patient Case • LB was started on vancomycin 125 mg VFT Q6h for 14 days on 7/11/13 • His route was changed to PO on 7/14/13 • His dose was changed to 250 mg PO Q6h on 7/15/13 • His diarrhea was resolving upon discharge on 7/24/13
Review of C. difficile • Good bacteria are essential for nutrition and immune response • C. difficile is increasing in incidence • More virulent strains are being discovered, caused by resistance • Risk factors include: • Antibiotic use • Health care environments • Advancing age • PPI use?
References • Clinical Pharmacology [Internet]. Tampa, (FL): Gold Standard, Inc. fidaxomicin;[Updated 2013 Jul 15;Cited 2013 Aug 6]; [about 3 screens]. Available from: http://www.clinicalpharmacology.com Registration and login required. • Louie T, Miller M, MullaneK, Shue Y, et al. Fidaxomicin versus Vancomycin for Clostridium difficile Infection. N Engl J Med [Internet]. 2011 [cited 2013 Aug 2]; 364:422-31. • LaMont JT. Clostridium difficile in adults: Epidemiology, microbiology, and pathophysiology.[Internet]. In: Calderwood S, Baron E, editors. UpToDate. Waltham (MA): UpToDate, Inc; 20103[cited 2013 Aug 3]. 4 p. Available from: http://www.uptodate.com Registration and login required. • Cohen S, Gerding D, Johnson S, Wilcox M, et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Disease Society of America (IDSA). Infection Control and Hospital Epidemiology [Internet]. 2010 May[cited 2013 Aug 2];31(5):431-55. Available from: http://www.idsociety.org Registration and login required • Clostridium difficile [Internet]. Atlanta(GA): Centers for Disease Control and Prevention; 2013 [cited 2013 Aug 4]: Available from: http://www.coc.gov/HAI/organisms/cdiff
References 6. Deshpande A, Pant C, Pasupuleti V, Hernandez A, et al. Association Between Proton Pump Inhibitor Therapy and Clostridium difficile Infection in a Meta-Analysis. Clinical Gastroenterology and Hepatology [Internet]. 2012 Mar [cited 2013 Aug 8]; 10(3):225-33. 7. Goldenberg JZ, Ma SSY, Saxton JD, Martzen MR, Vandvik PO, ThorlundK, GuyattGH, Johnston BC. Probiotics for the prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database of Systematic Reviews 2013, Issue 5. Art. No.: CD006095. DOI: 10.1002/14651858.CD006095.pub3. 8. Micromedex 2.0 Red Book [Internet]. Greenwood Village (CO): Truven Health Analytics Inc. c2013. fidaxomicin; [cited 2013 Aug 11]; [about 3 screens]. Available from: http://www.micromedex.com Registration and login required.