Download
1 / 20
230 likes | 635 Views
Clostridium difficile. Ricardo A. Caicedo, M.D. Pediatric Gastroenterology UPDATED JULY 2006. OBJECTIVES. Introduction Epidemiology Clinical spectrum Diagnosis Treatment Prevention. INTRODUCTION. Gram + bacillus Anaerobic Spore-forming Slow growing Difficult to culture

E N D
Clostridium difficile Ricardo A. Caicedo, M.D. Pediatric Gastroenterology UPDATED JULY 2006
OBJECTIVES • Introduction • Epidemiology • Clinical spectrum • Diagnosis • Treatment • Prevention
INTRODUCTION • Gram + bacillus • Anaerobic • Spore-forming • Slow growing • Difficultto culture • Historically…. • 1935: first described in fecal flora • healthy neonates • 1970s: toxins implicated in antibiotic-associated diarrhea and colitis JA Hobot University of Wales College of Medicine UK
FREQUENCY • Age-dependent • Neonates • High colonization rate (60-65%) • Usually asymptomatic carriers • Infants (1-24 m) • More symptomatic • Peak: 6-12 m • Children 3-18 y • Prevalence 5-8% • as in adults • Outbreaks • Nosocomial • Daycare centers McFarland LV et al (2000). JPGN 31(3):220-31.
C. difficile in the neonate • Susceptible to colonization • Immature intestinal microflora • Exposure to spores in the nursery • Rarely symptomatic • Immature mucosal inflammatory response • Gut epithelial toxin receptor defect • Maternal Ab • Absence of complex dietary substrates
PATHOGENESIS • Toxin-mediated • Toxin A (enterotoxin) • More biologically active • Toxin B (cytotoxin) • Diagnostic marker • Toxins bind to villus enterocyte receptors • Inflammation • Increased permeability • Increased secretion • Fibrin deposition • Activation of enteric NS Poutanen SM, Simor AE (2004) CMAJ 171(1):51-8. G
Disruption of normal microflora ANTIBIOTICS Altered mucin layer Prematurity Immunosuppression GI problems Short bowel Colonic stricture Hirschsprung’s IBD Co-infection RISK FACTORS
CLINICAL PRESENTATION Asymptomatic carrier Acute/protracted diarrhea Colitis Recurrent disease
Acute/protracted diarrhea • > 3 watery stools/d for > 2 days • Fluid content > 10 ml/kg/d • Typical duration: 2-9 days • Chronic diarrhea (>14 d) • 7 wks-19 m (Cooperstock M, 1990) • Other possible GI sx • Colicky abdominal pain • Abdominal distention • Vomiting • May or may not be associated with antibiotic use
Antibiotic-associated diarrhea • 4-18 days after first antibiotic dose (Ferroni A et al, 1997) • Almost any antimicrobial • Abx exposure not prerequisite for C. diff. disease • 78% symptomatic outpts had no abx for at least 1 m (Buenning DA et al, 1982) McFarland LV et al (2000). JPGN 31(3):220-31.
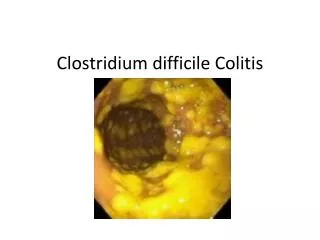
TYPES Pseudomembranous (PMC) Non-PMC Toxic megacolon SIGNS/Sx Profuse diarrhea Blood in stool Abdominal pain Crampy LQ tenderness Fever Leukocytosis/L shift C. difficile COLITIS
Pseudomembranous colitis From G. Ginsberg MD, Univ. Penn. www.endoatlas.com/ Composition: Fibrin WBCs and cell debris Mucus Adherent Raised 0.2-2 cm diameter
COMPLICATIONS • Dehydration • Protein-losing enteropathy • Hypoalbuminemia • Ascites/edema • Colon perforation • Shock (fulminant colitis) • Undernutrition • Recurrent infection
DIAGNOSIS NEJM (1994) 330:256. • Detection + clinical • Detection of organism or its toxin is not diagnostic by itself • If sx suggest C. diff. disease, but stool is negative, repeat stool assays • Stool assays • Gold standard = cytotoxin cell culture assay • Drawback: results can take up to 72 h • Culture on CCFA agar • EIA (rapid enzyme immunoassay) • Results within 24 h • PPV 100% when both toxins A and B tested (Kader H et al, Gastro., 1998) • Endoscopy – reserve for ill patients • Pseudomembranes specific for C. diff. • CT scan – less specific
TREATMENT • D/C inciting antibiotic if feasible • Antibiotic therapy • Metronidazole • Vancomycin (PO) • Bacitracin • Biotherapeutics • Probiotics • Cholestyramine • IVIG • Whole bowel irrigation • Avoid anti-motility agents
Treatment • METRONIDAZOLE • Pros: effective, less expensive • Cons: taste, side effects, emerging resistance • Dosing: 20-40 mg/kg/d div. BID-QID • VANCOMYCIN PO • Pros: better colonic absorption, few side effects • Cons: expensive, resistance, recurrence • Indications: severe PMC, recurrence, immunocompromised • Dosing: 40 mg/kg/d div. QID
PROBIOTICS LGG Saccharomyces boulardii N= 19 infants C. diff. + diarrhea PO yeast X 15 d, no abx Sx resolved in 95% within 1 wk Rectal infusion of stool from healthy donor Broth culture bacteria Cholestyramine Binds both C. diff. toxins Also binds vancomycin Tastes like sand/seawater Primary tx failure, but better at preventing relapse IVIG Successful in uncontrolled trials in adults Very limited data in children Colon irrigation N = 2 children(Liacouras C, Piccoli D, J Clin Gastro 1996) Treatment McFarland LV et al (2000). JPGN 31(3):220-31.
RECURRENCE • 15-57% after standard tx • Typically 2-8 wks after completion of tx • Mechanisms • Re-acquisition • Persistence of spores in colon • Resistant strains • Management options • PO Vanc • Probiotics • Cholestyramine • IVIG • Solution of fresh stool from healthy donor McFarland LV et al (2000). JPGN 31(3):220-31.
PREVENTION • Exclusion from daycare for duration of diarrhea • Avoid abx in 1st 2 m after PMC • Probiotics in pts with hx recurrent disease • Inpatients • Narrow spectrum and use of abx when possible • Strict handwashing and enteric or contact precautions • Alcohol based hand sanitizer is not sporicidal • Decontaminate colonoscopes • Sporicides = glutaraldehyde or sodium hypochlorite Brook I (2005). J Gastroenterol Hepatol. 20(2):182-6.
Rising rate and severity of C. difficile disease in U.S. • Emergence of new strain • Increased virulence • Increased resistance • Associated with use of fluoroquinolone antibiotics