Download
1 / 19
220 likes | 571 Views
Preventing Preterm Birth. Kerri Thompson Advisor: Dr. Eric Reynolds. Background. Preterm birth= infants delivered after 20wks and before 37wks gestation The incidence of preterm birth has increased; 12% of births in the U.S.

E N D
Preventing Preterm Birth Kerri Thompson Advisor: Dr. Eric Reynolds
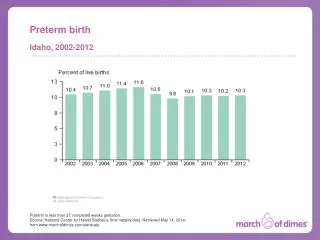
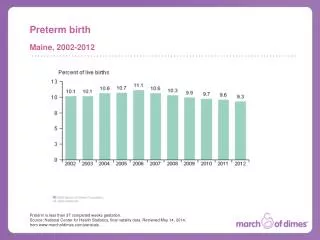
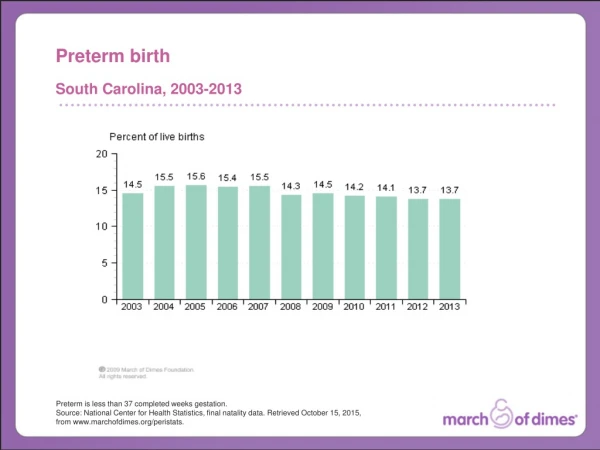
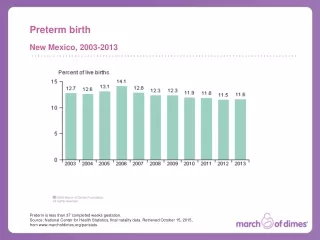
Background • Preterm birth= infants delivered after 20wks and before 37wks gestation • The incidence of preterm birth has increased; 12% of births in the U.S. • Account for the vast majority of perinatal mortality (around 80%) and about 50% of the long-term neurologic disability • Not well understood
Preterm Labor • Complex process- possible relationship between infection and inflammation with PTL • Braxton-Hicks contractions spontaneously resolve • Diagnosis is difficult but must be made in time it administer therapy • Consider contraindications to stopping PTL
Previous preterm birth Women pregnant with twins, etc. Uterine or cervical abnormalities i.e. incompetent cervix Premature membrane rupture Short time between pregnancies Diabetes, HTN Younger/older women African-American women have a 2-fold increase in PTB BMI<20 or obesity Infection Smoking, drinking, drugs Stess, working long hrs Late/no prenatal care 2nd trimester bleeding Risk Factors
Important info for PAs • Screen women for risk factors and enroll in PTL education programs by 18wks gestation if they are at risk • Seek immediate medical care if they experience signs of PTL • Basic signs are contractions every 10 minutes or more often, change in vaginal discharge like bleeding, pelvic pressure, low dull backache, cramping as with a period, or abdominal cramps with or without diarrhea
Prevention Goals • The goal of tocolytic therapy is to delay labor so the fetus can mature safely by delaying birth long enough to administer corticosteroids or to hopefully reach term • Steroids speed up the lung maturation to enable the infant to breathe better after birth • Allow time to treat maternal infection or transfer to a tertiary care facility better equipped for PTB • Poor understanding of mechanisms involving tocolytics, PTL, inadequate research
Treatment Options • Bedrest- fairly inexpensive, typically safe, easily available, may offer some benefit • Lateral recumbent position relieves pressure of the uterus on the maternal great vessels, augmenting uterine blood flow, enhancing right atrial return, and maternal cardiac output • Assoc. maximal oxygenation and nutrient availability may decrease prostaglandin production (thought to be 1° triggers of PTL) • Worry about clots, anxious/depressed feelings, not proven efficacy
Cervical Cerclage • Can be used to prevent PTD in structural cervical defects such as a weak cervix or a short cervical length on transvaginal ultrasonography • surgical procedure closing the bottom half of the endocervical canal with a stitch until the 37-38 week of pregnancy • Mixed results, may only be an appropriate choice for true cervical incompetence • Potential risks- premature contractions, membrane rupture, cervical infection, cervical laceration if not removed before delivery, and cervical dystocia (unable to dilate normally)
Antibiotic Treatment • Infection is a strong risk factor for PTL • Should be started as early as possible because once the inflammatory process has begun, stopping labor may be quite difficult or possibly inappropriate • In PPROM, may significantly reduce the risk for chorioamnionitis, delay delivery 48hrs to 7days, and reduce neonatal mortality • Data has been conflicting
Progesterone • Necessary part of a normal pregnancy • 17α-hydroxyprogesterone was shown to decrease the incidence of PTB and the # of infants weighing less than 2500g at birth • Rates of PTD at <37, <35, and <32 wks gestation were reduced, but ineffective in preventing PTB of twins in another study • Lower rates of necrotizing enterocolitis, need for supplemental oxygen, and intraventricular hemorrhage and no teratogenic/fetotoxic effects • ACOG recommends the use of progesterone supplementation should be restricted to women with a documented history of prior spontaneous PTD • Promising but limited information on benefit or harm
Magnesium Sulfate • First-line tocolytic is due to its familiarity, ease of use, and almost absence of serious maternal AEs • minor side effects- feeling hot/flushed, n/v, blurred/double vision, or lethargic • Lethargy, hypotonicity, and low Apgar scores are the primary side effects in neonates • Stops 96% of PTL without cervical changes and 75-85% with cervical changes • A meta-analysis showed no substantial effect on the proportion of women delivering within 48hrs
β-sympathomimetic • Terbutaline is β2-receptor specific which is the receptor causing uterine relaxation and has replaced ritodrine • If contractions continue after 2 treatments, most clinicians switch to Mag. Sulfate • SEs- flushing, tachycardia, palpitations, hypotension, cardiac arrhythmias, chest pain, EKG changes, and myocardial ischemia with the most common serious AE being pulmonary edema • β-agonists are better in prolonging pregnancy 3-7 days and increasing birth weight, but have not shown a significant reduction in perinatal M & M
Calcium Channel Blockers • Initial choice in Europe, but remain 2nd line treatment in the U.S. • Appeal- effectiveness, ease of oral administration, rapid onset of action, tolerable SE, & lack of known neonatal AE • Reduced # of women giving birth within 7 days of treatment and before 34wks of gestation, assoc. with a reduction in neonatal RDS, necrotizing enterocolitis, intraventricular hemorrhage, and neonatal jaundice • SE- dizziness, lightheadedness, HA, flushing, nausea, and transient hypotension • MgSO4 and Nifedipine should not be used together
Antiprostaglandin synthetase inhibitors • Prostaglandins are key components in the labor process • Indomethacin- nonspecific COX-1 & 2 inhibitor • Reduces the # of deliveries within 48hrs & before 37wks, but due to concern over the SEs, it is typically used only when other therapies fail • Fetus should be monitored for signs of ductal constriction or oligohydramnios and could mask chorioamnionitis and may independently increase the rate of NE and grade III to IV intraventricular hemorrhage • Compared with β-mimetics, MGSO4, and atosiban… indomethacin proved superior in tocolytic efficacy without an increase in neonatal or maternal morbidity
Oxytocin receptor blocker • Oxytocin is believed to play a role in human labor, but extent is controversial • Atosiban has been shown to have the same efficacy as other tocolytics but with fewer SE and has been successful as a maintenance therapy • SE- n/v, headaches, and chest pain, no known AE in the infant • Not enough data is available yet for atosiban to be widely accepted
Comparison • Pregnancy was prolonged more than 48 hours significantly more frequently in patients receiving nifedipine when compared to β-agonists • When compared to magnesium sulfate, there was no difference in efficacy, but nifedipine was better tolerated • When indirectly compared with atosiban, nifedipine is more effective and is assoc. with a significant reduction in RDS, but when directly compared the efficacy was the same, but the AE of nifedipine were significantly more
Conclusion • Until the controversy with indomethacin use is resolved and atosiban is better researched, nifedipine, a calcium channel blocker, appears to be the preferred tocolytic due to its efficacy and tolerability