Download
1 / 29
290 likes | 456 Views
Progestogens for Prevention of Preterm Birth. Prepared for: Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov. Outline of Material. Introduction to preterm birth, the goals of preterm birth prevention, and the use of progestogens Systematic review methods

E N D
Progestogens for Prevention ofPreterm Birth Prepared for: Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov
Outline of Material • Introduction to preterm birth, the goals of preterm birth prevention, and the use of progestogens • Systematic review methods • The clinical questions addressed by the comparative effectiveness review • Results of studies and evidence-based conclusions about effectiveness and adverse effects of progestogens • Gaps in knowledge and future research needs • What to discuss with patients and their caregivers Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
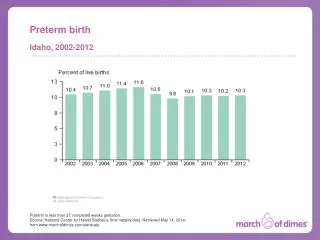
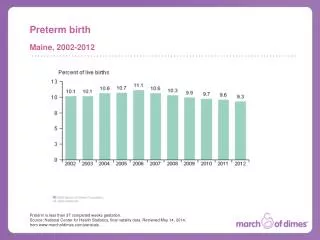
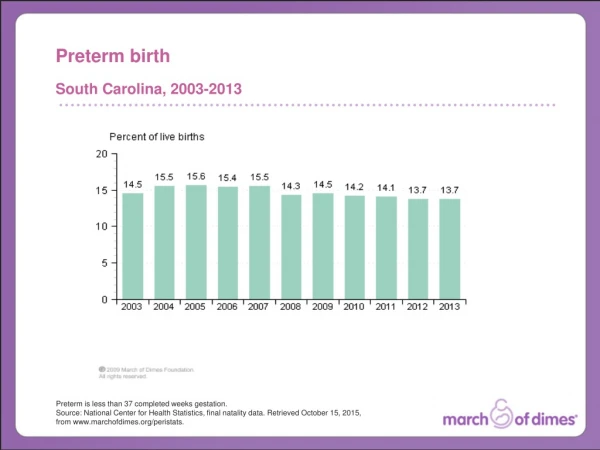
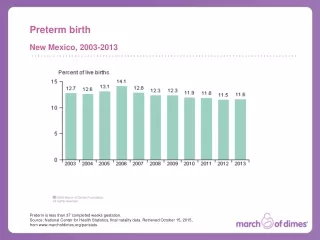
The Burden of Preterm Birth • Preterm birth is defined as birth prior to the 37th week of pregnancy. • Each year in the United States, 12.5 percent of births (representing more than 475,000 infants) occur preterm. • The risk of complications is related to how early the birth occurs. • The morbidity and mortality associated with preterm birth represent untold distress for families, as well as significant costs to patients, health care systems, and payers. • The estimated additional cost for neonatal care is $17,300 (2004 dollars) per preterm infant. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Risk Factors for Preterm Birth • Women known to be at risk for preterm birth include those with: • Prior preterm birth • Symptoms of preterm labor • Multiple gestations • Short cervix • Other: • Abdominal surgery • Previous or threatened spontaneous abortion • Uterine anomalies • Incompetent cervix Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Approaches to Prevention of Preterm Birth • The ultimate goals of preventing preterm birth are: • To eliminate the risks of neonatal death or complications • To prevent long-term health consequences • To promote normal childhood development • To reduce maternal complications • Interventions used once a woman has symptoms of preterm labor have not been reliable for preventing preterm birth. • Earlier interventions based on risk rather than symptoms are hoped to be more effective. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Progestogens for Preventing Preterm Birth (1 of 2) • Progesterone is a hormone that inhibits the uterus from contracting. It is involved in maintaining pregnancy, especially early in gestation. • Progesterone has been recommended for pregnant women with prior preterm birth. • This use is based on reviews of clinical research that indicated that progesterone can prolong pregnancy for women at risk of preterm birth, based on having a prior spontaneous preterm birth. • “Progestogen” is an inclusive term for substances with biologic activity similar to the endogenous hormone progesterone. Progestogens include: • Natural progesterone • Synthetic progesterone • Synthetic progestins that are similar but not identical in chemical structure Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Progestogens for Preventing Preterm Birth (2 of 2) • Formulations of progestogens have been approved by the U.S. Food and Drug Administration (FDA), but for indications other than prevention of preterm birth. These forms include: • Vaginal suppositories, gels, and caps • Oral formulations • A commercial formulation of a progestogen for intramuscular injection has been approved by the FDA for preterm birth prevention. • 17 alpha-hydroxyprogesterone caproate • Formulations of progestogens may be supplied by compounding pharmacies. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Agency for Healthcare Research and Quality (AHRQ) Comparative Effectiveness Review (CER) Development • Topics are nominated through a public process, which includes submissions from health care professionals, professional organizations, the private sector, policymakers, members of the public, and others. • A systematic review of all relevant clinical studies is conducted by independent researchers, funded by AHRQ, to synthesize the evidence in a report summarizing what is known and not known about the select clinical issue. The research questions and the results of the report are subject to expert input, peer review, and public comment. • The results of these reviews are summarized into Clinician Research Summaries and Consumer Research Summaries for use in decisionmaking and in discussions with patients. The Research Summaries and the full report, with Reference:s for included and excluded studies, are available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Rating the Strength of Evidence From the Comparative Effectiveness Review • The strength of evidence was classified into four broad categories: Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Clinical Questions Addressed by theComparative Effectiveness Review (1 of 2) • Although progestogen treatment to prevent preterm birth has been endorsed, there are still unanswered questions about effectiveness and safety. • Clinical questions addressed by the comparative effectiveness review included: • Does progestogen treatment—when compared with placebo, usual care, or other interventions—improve maternal or fetal/neonatal health outcomes? • What are the nature and frequency of maternal and child adverse effects of progestogen treatment? • How do effectiveness, adverse effects, and safety of progestogen treatment differ based on maternal risk factors for preterm birth? Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Clinical Questions Addressed by theComparative Effectiveness Review (2 of 2) • How do effectiveness, adverse effects, and safety of progestogen treatment differ based on the formulation, dose, frequency of administration, and gestational age at initiation or discontinuation of progestogen therapy? • How do effectiveness, acceptability, adherence, adverse effects, and safety of progestogen treatment differ based on the cointerventions used to prevent preterm birth and its consequences? Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Clinically Significant Outcomes of Interest in the Comparative Effectiveness Review (1 of 2) • Maternal and fetal/neonatal outcomes • Complications during pregnancy • For example: chorioamnionitis, antenatal hospitalizations, intrauterine growth restriction, preterm labor • Mode of birth and complications • For example: cesarean birth, surgical complications • Prematurity • Gestational age at birth • Birth weight, fetal and neonatal mortality • Postpartum and neonatal complications • For example: maternal postpartum hemorrhage, intraventricular hemorrhage • Longer term outcomes • For example: neurodevelopmental and future reproductive outcomes Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Clinically Significant Outcomes of Interest in the Comparative Effectiveness Review (2 of 2) • Maternal and child adverse effects • Complications during pregnancy • For example: allergic reactions, gestational diabetes • Mode of birth and complications • For example: unanticipated maternal harms • Postpartum and neonatal complications • For example: infection and sepsis • Longer term outcomes • For example: reproductive and neurodevelopmental adverse effects Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Potential Modifiers of Progestogen Effects on Preterm Birth Outcomes • Modifiers are characteristics that interact with the treatment to change the expected outcome, when compared with those without the characteristic. • Gestational age of prior spontaneous preterm birth • Number of prior spontaneous preterm births • Prior preterm premature rupture of membranes • Short cervix • Number of fetuses in multiple gestations • Preterm labor in the current pregnancy • Maternal age • Body mass index • Cerclage • Socioeconomics • Conception via reproductive technology Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Summary of Study Characteristics Evaluated in the Effectiveness Review: PICOTS • Population: Adult women at risk for preterm birth • All risk factors • Interventions: Progestogens • All formulations, routes, and doses • Comparators: Placebo or no active intervention • Outcomes: • Preterm birth, gestational age • Maternal, fetal, and neonatal health outcomes • Timing: Treatment initiated at any time point prior to 37 weeks • Setting: Community Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Studies Examining Progestogen Effects • In most studies, the specific risk factors of the treatment and control group patients were identified. These risk factors include: • Prior spontaneous preterm birth • Current multiple gestation (twins and triplets) • Short cervix • Threatened preterm labor • Varied risk factors (a variety of indications among the patients) • Unique indications (e.g., abdominal surgery, midtrimester amniocentesis, active military duty) Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Studies and Results by Indication (1 of 3) Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Studies and Results by Indication (2 of 3) Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Studies and Results by Indication (3 of 3) Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Summary of Benefits:According to Indication/Risk Group (1 of 3) • In women with current singleton pregnancies and a history of spontaneous preterm birth, progestogen treatment: • Reduces the risk of preterm birth by one-third (number needed to treat = 11) • Strength of Evidence = Moderate • May increase birth weight, but the summary result across studies is not statistically significant • Strength of Evidence = Moderate • Reduces neonatal mortality rates, with an absolute risk reduction of 1.7 percent (number needed to treat = 58) • Strength of Evidence = Low Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Summary of Benefits:According to Indication/Risk Group (2 of 3) • Women with short cervix may benefit from progestogen treatment (studies used vaginal formulations), but the size of the effect is not established. • Strength of Evidence = Low • In women with twin or triplet pregnancies there is no benefit of progestogen treatment. • Birth is not delayed. • Strength of Evidence = Moderate • Birth weights are not improved. • Strength of Evidence = Moderate • The evidence about mortality rates is insufficient to permit a summary estimate of the effect. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Summary of Benefits:According to Indication/Risk Group (3 of 3) • The present review found that progestogens may delay preterm birth in women with preterm labor, but the current evidence base is imprecise and insufficient to permit a conclusion about the effect. • The evidence is insufficient for all other indications. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Studies and Results Based on Formulation and Route of Administration The authors of the comparative effectiveness review analyzed published study data by organizing it according to formulation and route of administration: intramuscular, oral, and vaginal. The analysis did not differentiate studies according to indication. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Summary of Benefits: Effect of Formulation and Route of Administration • All formulations succeeded in reducing the risk of spontaneous preterm birth. • The evaluated studies were not differentiated according to risk factor. • The studies evaluated spontaneous preterm birth at 35 to 37 weeks. • No formulation was effective at reducing the risk for neonatal mortality. • However, the evidence is insufficient to support conclusions about the true benefits or effect sizes. • It is possible that differences associated with progestogen use arise solely from populations studied or other biases. • Head-to-head comparisons are needed to provide sufficient evidence to permit conclusions about the comparative effectiveness of these formulations. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Evidence About the Adverse Effectsof Progestogens • Study withdrawals were similar for treated and control groups. • The most common adverse effects were related to route of administration. • Injection site discomfort • Vaginal irritation • The evidence is insufficient to understand the short- and long-term maternal and fetal adverse effects. • Potential adverse events were not uniformly assessed in the clinical literature. • There are no registries to accumulate data on rare or long-term adverse effects for either mothers or children. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Effects of Modifiers of Outcomes and Safety • None of the studies of maternal characteristics had sufficient statistical precision and power to determine the effects of modifiers on benefits and adverse effects of progestogens. • No data inform whether effectiveness of progestogen treatment varies among women with prior preterm premature rupture of membranes, cerclage, uterine malformation, or conceptions via assisted reproduction technology when compared with other women. • No dose-finding studies focused on efficacy or effectiveness were identified in this review. • No literature addresses whether adherence or acceptability to patients varies by formulation, dose, or route. • For all the modifiers evaluated, the evidence is insufficient to guide care. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Conclusions About Benefits and Adverse Effects • For women with prior spontaneous preterm birth and current singleton pregnancies, progestogens reduce the risk of preterm birth. • Women with a short cervix may benefit, but the research is too limited to estimate the likelihood. • There is no benefit for women with multiple gestations. • For all other indications, the evidence is insufficient to guide care. • The incidence of rare adverse events is not known. • The effects of modifiers are unknown. • The evidence is insufficient to know whether progestogen use prevents morbidity or promotes normal childhood development. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
Gaps in Knowledge • The effectiveness review revealed areas where the evidence is inadequate to support decisionmaking that balances the benefits and adverse effects of progestogens used to prevent spontaneous preterm birth. • The thresholds where improved gestational age and birth weight translate into improved neonatal and childhood outcomes are not known. • The differences in effectiveness between different formulations and dosages, timing of initiation, and duration of treatment have not been studied in head-to-head comparisons. • The influence of potential modifiers (e.g., body mass index, short cervix) has not been determined. • The effects on maternal outcomes (e.g., prenatal hospitalization, tocolysis, gestational diabetes, hypertension) are not known. • Patient adherence to treatment and reasons for discontinuation are rarely reported or investigated. • Long-term risks are not known, and no surveillance database is available for reporting adverse events. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.
What To Discuss With Your Patientsand Their Caregivers • Progestogens reduce the risk of preterm birth for women who previously had a spontaneous preterm birth and who currently have a singleton pregnancy. They may also benefit women with a short cervix. They do not prevent preterm birth for multiple gestations. • There is little evidence about using progestogens for women with preterm labor or other risk factors for preterm birth. • The evidence about differences between the oral, injection, and vaginal methods for treatment is limited. • It is not known if progestogens will provide short- or long-term health benefits to the infant or mother, other than delaying birth, and there is little evidence about short- and long-term adverse effects. Likis FE, Andrews JC, Woodworth AL, et al. AHRQ Comparative Effectiveness Review No. 74. Available at www.effectivehealthcare.ahrq.gov/pretermbirth.cfm.