Download
1 / 29
290 likes | 314 Views
Learn about the Auto-HPSAs program for shortage designation assistance, criteria, and updates. Utilize designated facilities for automatic HPSA designation and review eligibility. Transparency, accountability, and parity are core principles. Stay informed on the upcoming national update.

E N D
Shortage Designation Modernization Project:Auto-HPSAs Janelle D. McCutchenDHEd, MPH, CHES Chief, Shortage Designation Branch Division of Policy and Shortage Designation Bureau of Health Workforce
Shortage Designations* Help Target Resources** *42 USC §254e(d)(1): “The Secretary shall determine health professional shortage areas in the States, publish a descriptive list of the areas, population groups, medical facilities, and other public facilities so designated, and at least annually review and, as necessary, revise such designations.” **List of programs is not exhaustive.
Current Auto-HPSA Scores Current Auto-HPSA Scores Current Participants and Those Awarded in 2019 • No changes to Auto-HPSAs have occurred • May be used for 2019 National Health Service Corps (NHSC) and Nurse Corps (NC) application cycles Will not be impacted by national update of HPSA scores May complete their service obligations-even if scores change. If eligible for a continuation-may be awarded as long as participants are working in a HPSA
National Health Service Corps: Substance Use Disorder (SUD) Investments • $225 million may be used to strengthen the substance use disorder workforce, of that some will be dedicated to: • Rural Communities Opioid Response • $45 million in loan repayment awards to rural communities with high opioid mortality rates • American Indian/Alaska Native • $15 million for SUD or traditional NHSC LRP awards to IHS, Tribal, and Urban Indian health care delivery sites https://bhw.hrsa.gov/loansscholarships/nhsc
Automatically Designated Facility HPSAs Using the statute and regulations, HRSA has deemed the following facility types as eligible for automatic HPSA designation: • Health Centers (funded under Sec. 330) • Health Center Look-Alikes • Tribally-Run Clinics • Urban Indian Organizations • Dual-Funded Tribal Health Centers • Federally-Run Indian Health Service Clinics • CMS-Certified Rural Health Clinics meeting NHSC site requirements
Auto-HPSAs compared to other HPSAs Similar but not the same Automatic Facility (Auto-HPSAs) Other HPSAs • Designation & scoring done online • Criteria used to first designate as HPSA • Criteria used to determine HPSA score • Scores range from 0-25 (26 for dental) • Designations are required to be reviewed and updated as necessary annually • Score of “0” is rare • Designation & scoring currently done manually • No application process necessary • Same criteria used to determine HPSA score as other HPSAs • Same scoring range used • HRSA has not historically required Auto-HPSA scores to be reviewed regularly; updates are requested by facility • Score of “0” more frequentand means low shortage or no data was available for scoring
Shortage Designation Modernization Project Core Principles TRANSPARENCY ACCOUNTABILITY PARITY The Shortage Designation Modernization Project utilizes the existing HPSA scoring criteria. No changes to the criteria have been made.
HPSA Scoring Criteria HPSA scores are based on a variety of criteria and range from 0 to 25 in the case of Primary Care and Mental Health, and 0 to 26 in the case of Dental Health. Primary Care 0-25 Mental Health 0-25 % of Population at 100% Federal Poverty Level Point Value % of Population at 100% Federal Poverty Level Point Value Double Weighted Population-to-Provider Ratio Point Value Double Weighted Population-to-Provider Ratio Point Value Double Weighted Infant Health Index Point Value (Based on IMR or LBW Rate) Water Fluoridation Status Point Value % of Population at 100% Federal Poverty Level Point Value Population-to-Provider Ratio Point Value Alcohol Abuse Prevalence Point Value Substance Abuse Prevalence Point Value Travel Time to Nearest Source of Care Point Values Travel Time to Nearest Source of Care Point Values HPSA Score (out of 25) HPSA Score (out of 26) Travel Time to Nearest Source of Care Point Values HPSA Score (out of 25) Elderly Ratio Point Value Youth Ratio Point Value Dental Health 0-26
National Update of Auto-HPSAs • Tentatively planned for this Spring/Summer (no sooner than April, no later than August) • Series of Auto-HPSA preview reports in advance • Raise awareness of Auto-HPSAs • Provide scoring transparency • Enable HRSA to provide technical assistance • Submit supplemental data to change Auto-HPSA scores • facility-specific data • fluoridation status, alcohol misuse rate and substance misuse rate data • Work with State Primary Care Offices (PCOs) to ensure provider data are correct
Auto-HPSA Working Group: Data Proposals Thank you to the Auto-HPSA Working Group: • Nathan Baugh (National Association of Rural Health Clinics) • Jennifer Harrison (Eastern Aleutian Tribes) • Debra Jahnke (Minnesota Department of Health) • Aleksandr Kladnitsky (Wisconsin Primary Health Care Association) • Maine Primary Care Association • Jyl Marden (California Consortium for Urban Indian Health) • Colleen Meiman (National Association of Community Health Centers) • Alan Morgan (National Rural Health Association) • Greg Nycz (Family Health Center of Marshfield) • Shelly Phillips (Association for Utah Community Health) • Thomas Rauner (Nebraska Division of Public Health) The Shortage Designation Modernization Project utilizes the existing HPSA scoring criteria. No changes to the criteria have been made.
Community Health Centers* Service area • Defined by zip codes in which 75% of a Auto-HPSA facility’s patients resideto create a Zip Code Tabulation Area (ZCTA)-based service area. (Source: 2017 UDS) DEFINITION • Population defined as low income population at or below 200% FPLin the service area. (Source: Census) • Providers defined as the count of eligible FTEs that serve Medicaid patients AND/OR provide services on a sliding fee scalein the service area. (Source: SDMS) Rural Health Clinics** Service area • Defined by census tracts intersecting with a 30 or 40 minute travel polygonto create service area. (Source: SDMS) DEFINITION • Population defined as low income population at or below 200% FPLin the service area. (Source: Census) • Providers defined as the count of eligible FTEs that serve Medicaid patients AND/OR provide services on a sliding fee scalein the service area. (Source: SDMS) I/T/Us** Service area • Defined by census tracts intersecting with a 30 or 40 minute travel polygonto create service area. (Source: SDMS) DEFINITION • Population defined as total population of American Indian and Alaska Native alone or in combination with one or more races (when available) in the service area. (Source: Census) • Providers defined as the count of eligible FTEs that serve the American Indian and Alaska Nativepopulations within the service area. (Source: SDMS) *Scoring will be at the organizational level. **Following the National Update, RHCs and ITUs may provide facility-level data to be rescored.
Dual-Eligible Organizations • Being scored as FQHCs with their UDS data. • In part, why the supplemental data for ITUs is critical.
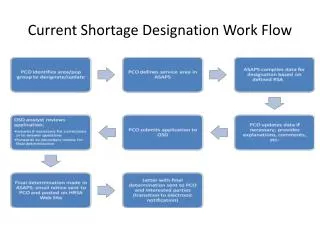
Determining the Default Service Area • Site is geocoded • 30 or 40 min travel polygon is drawn around the site • Census tracts (CT) that overlap the travel polygon are identified and saved as the service area • All usable providers located in the CT service area are identified NOTE: A provider used in the population to provider ratio can be more than 30 or 40 minutes away from the site. *Default Service Area is used for ITUs, RHCs and FQHCs/LALs that have not reported UDS data.
Ratio of Population to ProvidersWhich Providers Count? Primary Care Dental Health Mental Health Includes: • Psychiatrists, and may include other Core Mental Health (CMH) providers, such as: • Clinical Psychologists • Clinical Social Workers • Psychiatric Nurse Specialists • Marriage & Family Therapists Includes Doctors of Medicine (MD) and Doctors of Osteopathy (DO) who provide services in the following specialties: • Family Practice • Internal Medicine • Obstetrics and Gynecology • Pediatrics Includes: • Dentists, and takes into account • Dental Auxiliaries Dental auxiliaries are defined as any non-dentist staff employed by the dentist to assist in the operation of the practice. Note: Providers solely engaged in administration, research or training are excluded.
Providers Used for Population to Provider Ratios • Service Area Approach • Includes all eligible providers in your organization’s service area • Not just your organization • If service area crosses state lines, providers may be from another state • A provider can be more than 30 or 40 minutes away from the site. • State Primary Care Office (PCO) is responsible for the provider data
If there are no providers in the population to provider spreadsheet how is the subscore being calculated? Primary Care Dental Health
If there are no providers in the population to provider spreadsheet how is the subscore being calculated? (continued) Mental Health
Rural Health Clinics* Service area • Defined by census tracts intersecting with a 30 or 40 minute travel polygon to create service area. (Source: SDMS) DEFINITION • Out of the population in the service area, the count of individuals at or below 100% FPL divided by the total population for whom poverty is determined. (Source: Census) Community Health Centers Service area • Not used DEFINITION • The percent of population of patients served with known incomeat or below 100% FPL (Source: 2017 UDS) I/T/Us* Service area • Defined by census tracts intersecting with a 30 or 40 minute travel polygon to create service area. (Source: SDMS) DEFINITION • Out of the population in the service area, the count of individuals at or below 100% FPL divided by the total population for whom poverty is determined. (Source: Census) *Following the National Update, RHCs and ITUs may provide facility-level data to be rescored.
Community Health Centers • DEFINITION • The nearest provider that serves Medicaid patients AND provides services on a sliding fee scalewho is not in an over utilized* area. (Source: SDMS) • I/T/Us • DEFINITION • The nearest provider that serves American Indian/Alaska Native populations who is not in an over utilized* area. (Source: SDMS) • Rural Health Clinics • DEFINITION • The nearest provider that serves Medicaid patients AND provides services on a sliding fee scalewho is not in an over utilized* area. (Source: SDMS) • *To determine overutilization: a 30-40 minute travel polygon will be drawn around each provider based on private • transportation to create an area from which the population and provider data will be pulled. (Source: SDMS) • A provider will be considered over-utilized if the population to provider ratio is greater than: • Primary Care: 2,000:1 • Dental Health: 3,000:1 • Mental Health Note: Following the national update, State Primary Care Offices will be able to change NSCs • Providers will be considered over-utilized if the population-to-provider ratio for psychiatrists ≥ 10,000:1 and the population-to-provider ratio for Core Mental Health providers is ≥ 3,000:1; • If there is no data on Core Mental Health providers other than psychiatrists or the Core Mental Health other than psychiatrists FTE = 0, providers will be • considered over utilized if the population-to-provider ratio for psychiatrists is ≥20,000:1.x
Rural Health Clinics DEFINITION • IMR: Out of the total population, the count of infant deaths divided by the total number of infant births for the county/counties in which the Auto-HPSA ‘s service area intersects. Scaled by 1,000. (Source: CDC) • LBW: Out of the total population, the count of low birth weight births divided by the total number of infant births for the county/counties in which the Auto-HPSA’s service area intersects. Scaled by 100. (Source: CDC) I/T/Us DEFINITION • IMR: Out of the total population, the count of infant deaths divided by the total number of infant births for thecounty/counties in which the Auto-HPSA ‘s service area intersects. Scaled by 1,000. (Source: CDC) • LBW: Out of the total population, the count of low birth weight births divided by the total number of infant births for the county/counties in which the Auto-HPSA’s service area intersects. Scaled by 100. (Source: CDC) Community Health Centers DEFINITION • IMR: Out of the total population, the count of infant deaths divided by the total number of infant births for the county/counties in which the Auto-HPSA ‘s service area intersects. Scaled by 1,000. (Source: CDC) • LBW: Out of the total population, the count of low birth weight births divided by the total number of infant births for the county/counties in which the Auto-HPSA’s service area intersects. Scaled by 100. (Source: CDC)
Rural Health Clinics DEFINITION • Score default to “0”. I/T/Us DEFINITION • Score default to “0”. Community Health Centers DEFINITION • Score default to “0”. • Following the National Update tentatively scheduled for spring/summer 2019, all Auto-HPSA facilities may provide supplemental information for a point to be awarded, where warranted. • To receive a score of 1, must provide data showing that less than 50% of the population has access to fluoridated water
I/T/Us* DEFINITION • The count of individuals younger than 18, or 65 and older, divided by the count of adults age 18-64. (Source: Census) Rural Health Clinics* DEFINITION • The count of individuals younger than 18, or 65 and older, divided by the count of adults age 18-64. (Source: Census) Community Health Centers DEFINITION • Out of the total unduplicated patient population, the count of individuals younger than 18, or 65 and older, divided by the count of adults age 18-64. (Source: 2017 UDS) *Following the National Update, RHCs and ITUs may provide facility-level data.
I/T/Us DEFINITION • Score default to “0”. Community Health Centers DEFINITION • Score default to “0”. Rural Health Clinics DEFINITION • Score default to “0”. Following the National Update tentatively scheduled for spring/summer2019, all Auto-HPSA facilities may provide supplemental information for a point to be awarded, where warranted. • To receive a score of 1, must provide data showing that the alcohol misuse rate is in the worst quartile for the nation, region or state • To receive a score of 1, must provide data showing that the substance misuse rate is in the worst quartile for the nation, region or state
Supplemental Data: Following the National Update* State Primary Care Offices ITUs/RHCs FQHCs and FQHC LALs • Zip codes in which 75% of the Auto-HPSA facility’s patients reside • The percent of population of patients served with known income at or below 100% FPL • Out of the total unduplicated patient population, the count of individuals younger than 18, or 65 and older, divided by the count of adults age 18-64 • Water Fluoridation • Alcohol Misuse Rate • Substance Misuse Rate • Nearest Source of Care • Water Fluoridation • Alcohol Misuse Rate • Substance Misuse Rate • Water Fluoridation • Alcohol Misuse Rate • Substance Misuse Rate Facility-specific Data • Reporting period: calendar year • January 1, 2017-December 31, 2017 • January 1, 2018-December 31, 2018 (Preferable) • The fluoridation, alcohol misuse and substance misuse data do not need to mirror the HRSA-created service area. • However, the information submitted should reflect the service area (i.e., be based on the organization’s address and sites) and represent a minimum 12 month reporting period. *Data will be submitted via online portal. Data will be accepted on a continual basis.
What Organizations Can Do Now • Focus on supplemental data • Assist PCOs with provider data • Make sure contact information is correct in EHBs or BHW Portal/BMISS system
To Whom to Direct Questions • Project itself (purpose, timeline, etc.): SDMP@HRSA.gov • Data shown on Update Preview Report: State PCO • Provider data: State PCO • Update preview scores: State PCO • Supplemental data: State PCO • Score or rescore* before the national update: SDB@HRSA.gov • State Primary Care Offices:https://bhw.hrsa.gov/shortage-designation/hpsa/primary-care-offices Project Website: https://bhw.hrsa.gov/sdmp *Tentativelast day SDB will receive requests: April 1, 2019.
Shortage Designation Modernization Project Summary • No changes to HPSA scores have occurred at this time. • Current participants will not be impacted. • National update is tentatively planned for spring/summer 2019. • There are things that organizations can do to change their scores. • Before the update takes place: • Collect facility-specific • Collect supplemental data • Work with State Primary Care Offices on the provider data • Following the national update • Submit facility-specific and supplemental data • Note: 2018 UDS data will be added to the system so FQHCs and FQHCs LAL may request rescores, but the date on which the data will be available in our system has not yet been determined. • Contact SDMP@HRSA.gov with questions.
Connect with HRSA To learn more about our agency, visit www.HRSA.gov Sign up for the HRSA eNews FOLLOW US: