Download
1 / 35
440 likes | 1.28k Views
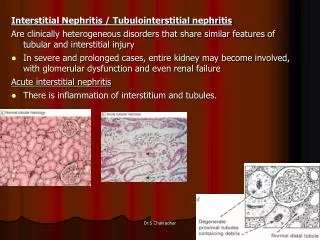
Acute Interstitial Nephritis. ?. Etiology. A review of three series with a total of 128 patients reported the following distribution of causes of acute interstitial nephritis : Drugs, with antibiotics responsible for one-third of these cases — 71 % Infection-related — 15 % Idiopathic — 8 %

E N D
Etiology • A review of three series with a total of 128 patients reported the following distribution of causes of acute interstitial nephritis : • Drugs, with antibiotics responsible for one-third of these cases — 71 % • Infection-related — 15 % • Idiopathic — 8 % • Tubulointerstitial nephritis and uveitis (TINU) syndrome (5 %) • Sarcoidosis — 1 %
Drug Induced AIN • The most common drug causes of AIN include: • NSAIDs, including selective COX-2 inhibitors • Penicillins and cephalosporins • Rifampin • Sulfonamides, including TMP-SMX. • Furosemide, bumetanide, thiazide-type diuretics • Ciprofloxacin >>other quinolones • Cimetidine >> other H2 blockers • Allopurinol • PPIs- omeprazole and lansoprazole • Indinavir • 5-ASA (eg, mesalamine) • Unifying factor-?
Infection Induced AIN • Infections — • Legionella • Leptospirosis • Cytomegalovirus • Streptococci • Many other bacterial, viral, and other infections have been associated with acute interstitial nephritis, including infection with: • Corynebacterium diphtheriae, • Epstein-Barr virus, • Yersinia, • Polyomavirus
Autoimmune Disorders • Numerous autoimmune disorders have been associated with AIN. These include: • Sarcoidosis, • Sjogren's syndrome, and others. • In addition, patients with: • SLE • Wegener's granulomatosis • often have an AIN accompanying the characteristic glomerular disease and, rarely, present with AIN in the absence of glomerular disease
Clinical Presentation • Acute or subacute onset of nausea, vomiting, malaise, and/or no symptoms. • The urine sediment -WBC, RBC, and WBC casts; • Eosinophiluria- >1%-- • also found with atheroemboli, GNs, prostatitis • Usually normal or only mildly increased protein excretion (less than 1 g/day). • Onset of the disorder ranges from 3-5 days with a 2nd exposure to the offending agent, to as long as several weeks with a first exposure. • However, the latent period may be as short as one day with rifampin or as long as 18 months with a NSAID
Clinical Presentation • Allergic-type symptoms • Rash — 15 % • Fever — 27 % • Eosinophilia — 23 % • Triad of rash, fever, and eosinophilia — 10 %
Clinical PresentationLaboratory • Laboratory — some combo of the following, with some variation based upon the underlying cause: • An acute rise in SCr, which (if drug-induced) is temporally related to administration of the offending drug. • Eosinophilia and eosinophiluria. • Except NSAID AIN-- fever, rash, and eosinophilia are typically absent • A urine sediment that usually reveals WBCs, RBCs, and WBC casts • Normal or only mildly increased protein excretion (< 1 g/day) • Concurrent nephrotic syndrome due to minimal change disease can be seen with NSAIDs and in selected cases induced by ampicillin, rifampin, interferon, or ranitidine • Signs of tubulointerstitial damage, such as the Fanconi syndrome and RTAs
Clinical PresentationLaboratory- 2008 KI • Typically think pyuria with urine eos, no heme, and allergic symptoms, but • 18% of patients do NOT have pyuria • Incidence of hematuria essentially equivalent to pyuria, and • Double the rate of eosinophilia, rash, or fever (approximately)
DiagnosisNon-Invasive • Gallium scanning • Diffuse, intense, bilateral uptake, consistent with the interstitial inflammatory infiltrate. • Although similar findings can occasionally be found in other disorders, the gallium scan is almost always negative in acute tubular necrosis, • A positive gallium scan is suggestive of AIN in the presence of the above characteristic findings. • A negative scan does not preclude the diagnosis, since false negative results can be seen
DiagnosisInvasive • Renal Biopsy • ? Use 20 gauge to limit complication risk
PrognosisDo we need to treat? • Acute dialysis is often required, but only about 10 percent of patients remain dialysis-dependent • Recovery of kidney function is often incomplete with persistent elevation of the Scr concentration in up to 40 percent of patients. In a review of published series of AIN: • In pts with a peak serum creatinine >5, the serum creatinine at the end of follow-up was less than 1.2 (50%) and 1.7 mg/dL (69%) • The final serum creatinine concentration did not correlate with the maximum value during AIN. • Clinical indicators of a decreased likelihood of recovery include : • Prolonged renal failure (greater than three weeks), • AIN associated with NSAID use, and • Certain histologic findings--including interstitial granulomas, interstitial fibrosis, and tubular atrophy (but data variable)
PrognosisCan you use peak Scr to determine the high risk group?
TreatmentSteroids • Theoretical Construct • Most cases of AIN are allergic reactions as suggested by the following: • The majority of the immune reactions are directly to drugs or drug-induced antigens; • Systemic manifestations of hypersensitivity are often present; • AIN is not a dose-dependent phenomenon and only a small percentage of patients develop the condition; • AIN typically improves following cessation of the drug; and • AIN may rapidly recur with accidental re-exposure to the drug or a closely related antigen. • T-cells may have an important pathogenetic role in the development of AIN as suggested from the following observations: • The timeframe of illness presentation, • 10 to 14 days after exposure to the drug, • is typical of a T-cell mediated syndrome; • the interstitial infiltrate in the kidney is composed primarily of lymphocyte • most patients demonstrate activation of lymphocytes against drug haptens
TreatmentOnly two controlled trials • American Journal of Medicine,1978--14 patients with methicillin-induced AIN, avg Scr of >8 mg/dL. 8 treated/6 observed
TreatmentOnly two controlled trials • Pusey, et al; Q J Med • Treated 7 of 9 patients with steroids- treatment group had a better outcome
TreatmentRetrospective 1990--27 patients with biopsy-proven AIN; 15 were drug-induced (1 methicillin, 2 ampicillin, 3 NSAIDS, 3 cimetidine,and the rest other), 9 infection, and 3 idiopathic • The 10 patients who did not improve following discontinuation of the drug or treatment of the infection (cause of AIN not specified) were given steroids within 5 to 20 days of biopsy (IV methylprednisolone 3 g/day for three days, or oral prednisone 40 to 60 mg/day for three to four weeks). • In six patients, serum creatinine normalized within approximately one month, and the remaining four had partial improvement in kidney function
TreatmentRetrospectiveEarly Steroid Treatment, KI 2008 • Strongly suggests that steroid treatment is indicated in DI-AIN and that it should be started immediately or soon after the diagnosis to avoid the risk of incomplete renal function recovery. • No significant side effects attributable to steroids were observed, probably due to the short duration of the treatment (8–12 weeks). • If offending agent simply d/cd, initial improvement is frequently exhausted and many patients will exhibit chronic renal insufficiency as a consequence of a DI-AIN episode. • Focus on the importance of an even mildly reduced renal function, both in terms of a future progression into end-stage renal failure and of an increased risk of cardiovascular events.
TreatmentRetrospectiveEarly Steroid Treatment, KI 2008 • 52 patients were treated with steroids 23±17 (range 2–68) days after the withdrawal of the offending drug (Group 1). • Although steroid doses and duration of the treatment were not uniform due to the multi-center character of the study, the most common scheme of treatment consisted of: • IV pulses of prednisone (250–500 mg daily for 3–4 consecutive days) followed by oral prednisone (1 mg/kg/day) tapering off over 8–12 weeks. • The remaining 9 patients did not receive steroids (Group 2).
Further Baseline Characteristics • Notice • Average pre-treatment creatinines approximately 5 • Required < two weeks of therapy on average
Non-responders versus responders to steroid therapyArgue for early treatment
Non-responders versus respondersHow quickly do you need to treat?
Non-responders versus respondersWhen will you see a response?4-6 weeks and both curves flatten
Non-responders versus respondersWhat are the risks? No significant side effects attributable to steroids were observed, probably due to the short duration of the treatment (8–12 weeks).
Explanation by steroid “defenders” Very advanced disease 58% either on dialysis or started within one week of biopsy 44% were NSAID related Believed to be less steroid responsive But subgroup analysis in this study showed no difference Clarkson, NDT 2004A similarly sized negative study
Which drug is associated with which profile?Methacillin, NSAIDs, Other Medications
Which drug is associated with which profile?Methacillin, NSAIDs, Other Medications Methacillin Other NSAIDS
? • 4 major categories of etiologies • 11 major drug categories • Typical urinary findings. Hematuria? • Percent of patients with classic allergic manifestations • How is NSAID associated AIN different? • What is the usual outcome of AIN? • Does the peak Scr tell you anything about the prognosis? • How quickly must you treat if you are going to see benefit? • When do you see a response from steroids? • When should you throw in the towel on steroids?