Download
1 / 54
540 likes | 696 Views
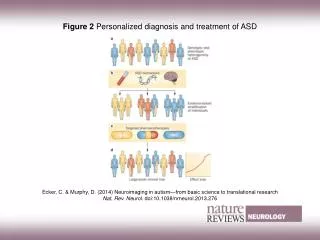
A Personalized Assessment and Treatment Model for Individuals with a Diagnosis of an Autism Spectrum Disorder: Asperger Syndrome January 24 and 25, 2013 Raymond W. DuCharme, PhD. Broader Definition, Autism Cases per 10,000 U.S. children More Cases

E N D
A Personalized Assessment and Treatment Model for Individuals with a Diagnosis of an Autism Spectrum Disorder: Asperger Syndrome January 24 and 25, 2013 Raymond W. DuCharme, PhD
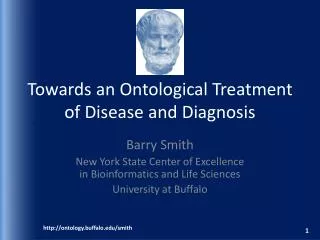
Broader Definition,Autism Cases per 10,000 U.S. children More Cases For decades autism was considered rare, perhaps a form of schizo- -- 100 phrenia. Rigorous definition in psychiatric manuals began in 1980 but broadened to “autism spectrum disorder” by 1994. As a result, more -- 80 andmore U.S. children were diagnosed, prompting schools to offer special education, parents to call for better treatments and practitioners -- 60 to offer an increasingly array of unapproved therapies. -- 40-- 20 -- 0 | o | | | | o | o | | 1940 1950 1960 1970 1980 1990 2000 2010 |-----------------------------------------------| | 1943 Autism1980 Autism first 1987 Category changed to1990 Autism first tracked1994 Autistic disorder, popularly defined designated as its own“autistic disorder” in revised under the Individuals with known as Autism spectrumdisorder, category, infantile autism, DSM-III; eight of 16 criteria Disabilities Education Act, is defined more broadly in DSM-IV to in DSM-III (Diagnostic and had to be met for a diagnosis. indicating need for special include syndromes such as Asperger’s; Statistical Manual of Mental education. only six diagnostic criteria had to be met. Disorders, third edition). The Learning Clinic January 2013
Asperger Syndrome Criteria The Learning Clinic January 2013
Asperger Syndrome Criteria Pragmatic language skill deficits not part of DSM-IV or ICD-10 criteria but should be included for differential diagnosis. The Learning Clinic January 2013
The lack of a well-defined diagnostic nosology results in questionable validity for research. If there is a continuum of degrees of impairment, developmental delays, and problematic self-regulation for each subtype of Autism, then each subtype needs to be separated for reliable interpretation of research outcomes. Most of the 2012 studies I reviewed failed to distinguish between subtypes. The studies bifurcated individuals into two groups High Functioning Autism (HFA) and Low Functioning Autism (LFA) or “blended” individuals into one group with a “typical developing group” for comparison. In most cases studies relied on small samples or large groups with small sub-samples of age, sex, and undifferentiated diagnoses. These threats to validity yield concern about the application of findings in treatment. The Learning Clinic January 2013
Key question that needs to be resolved prior to treatment planning: Is Autism Spectrum Disorder (ASD) a Phenotype or a Dimensional Structure of Symptoms? Corollary Questions: • What is the validity of the separate nosologic types of ASD? (Autism vs. High Functioning Autism vs. PDD-NOS vs. Asperger Syndrome) • Are the subtype diagnoses Quantitatively distinct (phenotypes) orQualitative manifestations of the same disorder? There is no clear empirical data to answer these basic questions at this time. The current trend in the literature is toward the acceptance of the concept of an Autism continuum without empirical support for the concept. The Learning Clinic January 2013
Some generalizations may be drawn however: ASD cluster scores in research studies indicate that a diagnosis of ASD and low IQ (< 75) scores will reveal problematic performance on: • Theory of Mind (ToM) • Attribution Tasks • Divided Attention Social Skills and Adaptive Behavior composite scores are down by 2 sd (SD=16.9) for this LFA group. The stronger the “cognitive make-up” measured high IQ scores, the better the scores by individuals on such tasks. Scores for the cluster of ASD did differentiate ASD from other clinical diagnoses, but did not differentiate quantitatively distinct phenotypes: Autism, HFA, PDD-NOS, or Asperger Syndrome. The Learning Clinic January 2013
Differential Diagnosis Asperger Syndrome vs. Autism – 75% IQ below 75 Verbal IQ – normal or above Developmental skills delayed Later onset of symptoms throughout development Academic competencies < LD Avoids social contacts specifically Math Early onset of developmental Wants relationships with peers delays Lack of social reciprocity Impaired social judgment Narrow focus of interest Early delayed language Perceived as bright, even development gifted early Long-term support usually Prognosis is positive for IL required Co occuring Diagnoses: Anxiety D/O Deppression Oppositional – Defiant D/O LD The Learning Clinic January 2013
Neuroatypical Learners • What interferes with the student development of educational competencies and cause special needs classification? • Neuroatypical factors specifically associated with LD and Autism Spectrum Disorders are discussed in Neurology of Cognitive and Behavior Disorders by Devinsky and D’Espisito (2004). The Learning Clinic January 2013
Functional brain imaging and electrophysiological studies indicate right brain hemisphere dominance over critical factors that influence how we experience “self” and therefore how we present to others, learn social skills and behavioral expectations. • Right hemisphere dominance controls: • self-recognition of one’s own face, ability to identify and describe feelings, our level of depersonalization, lack of sense of self, fear, grief, crying, morbid thoughts, ecstatic feelings The Learning Clinic January 2013
. . .and the . . . • ability to connect relationships between past and current experience. (source memory) • tangential thought, rambling, vague, loquacious speech The Learning Clinic January 2013
Volition (will) is modulated by right hemisphere function as is: • the ability to select and decide to take action • hold information in a fixed position in the mind in order to compare and contrast data • insight into consequences of actions • response to information directed at others versus self The Learning Clinic January 2013
The right hemisphere disorders can impair social awareness and behavior i.e. inability to comprehend emotional and social cues. Such impairment can cause lack of social greeting, eye contact and facial expression. • A person may have a normal to high IQ but lack the social pragmatic skills needed for social interactions, friendship and close personal relationships and motivation for social acceptance. • Impaired verbal communication of nonverbal affective signals • Impaired higher level inferential reasoning (figures of speech, sarcasm) The Learning Clinic January 2013
The lack of prosodic communication and impoverished gestural behavior are also evident. Flat affect, impaired awareness and responsiveness to social context is evident. • Poor arithmetic and visuo-spatial skills are also evident with impaired right hemisphere function. • demonstrate motor persistence • ability to perform two motor acts simultaneously . . . The Learning Clinic January 2013
Differential Diagnosis The Learning Clinic January 2013
Chart of Comparative Symptoms The Learning Clinic January 2013
Diagnostic Characteristics The Learning Clinic January 2013
Medications Cognitive Functioning The Learning Clinic January 2013
Age / Time Psychological Symptoms The Learning Clinic January 2013
Grade Clinical Symptoms and Learning Disabilities The Learning Clinic January 2013
Which Asperger Symptoms Compete with Independence? Age Degree of Anosognosia Over time, symptoms become egosyntonic The Learning Clinic January 2013
Personalized Treatment Model (PTM) requires identifying idiosyncrasies in each person’s general diagnosis that is relevant to predicted treatment outcomes. This PTM approach to treatment indicates the following three part focus for treatment: I. Psychopharmacological Management: • Genotyping to identify open or deficient pathways to drug metabolism and given medication options • Co-occurring conditions require treatment triage to maximize generalizations. • Number of discontinued medication trials • Historical polypharmacy • Dose changes through and over time • Medication synergies • Unintended outcomes from particular prescriptive drug use – weight gain, cognitive function interference The Learning Clinic January 2013
AS or PDD:NOS DiagnosisN = 21 The Learning Clinic January 2013
Autistic Spectrum DisorderN = 21 The Learning Clinic January 2013
All DiagnosesN = 32 The Learning Clinic January 2013
Dysfunctional Metabolization by Genetic PathwaysTotal Sample = 32 The Learning Clinic January 2013
Diagnostic Categories of Students with Abnormal Metabolization of 1 or More Genetic Pathways The Learning Clinic January 2013
Diagnostic Categories of Students with Abnormal Metabolization of 1 or More Genetic Pathways /Continued The Learning Clinic January 2013 38
Percentage of Medication Metabolized thru 2D6 The Learning Clinic January 2013
Goals Short-termobjectives focus: self-regulation resiliency Intermediatefunctional social judgment disclosure interpersonal communication Long-term family separation and individuation The Learning Clinic January 2013
Other Developmental Issues • Deviation from normal development • Do not “Outgrow” Developmental Deficits • Stress Impairs Performance • Co-Morbid Diagnoses Impairs Overall Functioning The Learning Clinic January 2013
Competing Clinical Behaviors • Perseveration • Obsessive Thought • Rigid Cognitive Style • Inability to Shift from “Personal View” to Data - Based Decision The Learning Clinic January 2013
Competing Clinical Behaviors / Continued • Confabulation • Affirming False Information • “Stealing” • Sexually Inappropriate Actions and Statements The Learning Clinic January 2013
Competing Clinical Behaviors / Continued • Violation of Boundaries • Cognitive Disorientation and Distortion The Learning Clinic January 2013
II. Therapeutic Needs for Management: • Social/Developmental atypicalities • Specific developmental strengths and deficits • Family history of DSM diagnoses • Clinical service history: individual, group, family, extended family therapy, partial hospital care, hospitalization • Specific family stressors • Treatment methods used and outcomes: CBT, Family Systems, Child-Parent Interactive Therapy, etc. • Fit of treatment approaches to clinical diagnoses, as perceived by family and child • GAF and Prognosis • Genetic markers associated with current diagnoses The Learning Clinic January 2013
III. Special Education Services A. Student Role Performance • Assessment through time and over time • Reliability of observations (in-vivo) teacher, mother, father, self • Targeted performance over time - minus baseline data = treatment benefit B. Level of intervention for in-school services through time and over time, • e.g., full inclusion, partial special classroom, shadow monitor, full special class, in-home supports, day outplacement, residential placement C. Evidence-based outcomes plus unintended outcomes D. Evidence of communication with parents E. Evidence of collaboration among professional disciplines: pediatrician, psychiatrist, developmental specialist, special educator, speech and language specialist, other . . . The Learning Clinic January 2013
F. Evidence of cohesive treatment and integrated services particular to an ASD individual’s requirements G. Academic modifications: evidence-based procedures such as teacher verbal or visual demonstration, rehearsal, prompting, redirection strategies, backwards chaining for sequential instruction, active learning instructional methods, Virtual Lab and CAI instruction. H. School and classroom ecology designed to structure support and elicit student role behaviors for individuals with ASD diagnoses. I. Safe school orientation operationalized to provide standards of accountability for staff and students regarding bullying, victimization, mutual respect and peer support The Learning Clinic January 2013
J. IEP written with personalized strategies to accommodate idiosyncrasies in student strengths and deficiencies with related assessment protocols: 1. Student role performance 2. Measures of retained academic skills 3. Measured ability to apply knowledge to real world problems 4. Self-regulation and classroom performance commensurate with the individual’s developmental age 5. IEP fit with assessed transition to post-high school plan, e.g., social judgment, pragmatic language skills, self-regulation, college experience, vocational experience, independent living skills, and experience with competitive employment (TILSA) The Learning Clinic January 2013
And IQ scores in another study accounted for more differences between groups than diagnoses (Rodman, J.L. et al, 2010) on measures of object exploration, diversity of play, and turn-taking tasks in young children. Criteria for Comprehensive Treatment Models for Individuals with ASD (J. Autism and Dev Disorders (2010) ODOM, et al) describe an evaluation system endorsed by the American Evaluation Association (2008). The Learning Clinic January 2013