Download
1 / 23
300 likes | 506 Views
Experimental Cancer Medicine Centres in the United Kingdom – A Framework for Translating the Results of Basic Science into Patient Benefit - Professor Herbie Newell and Dr Mags Sara -16 June 2007. Translational Research. “The exploitation of basic research for patient benefit”.

E N D
Experimental Cancer Medicine Centres in the United Kingdom–A Framework for Translating the Results of Basic Science into Patient Benefit- Professor Herbie Newell and Dr Mags Sara -16 June 2007
Translational Research “The exploitation of basic research for patient benefit”
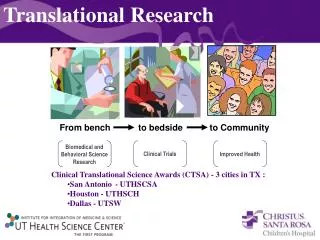
The Iterative Translational Research Cycle Patient - Bed Samples for drug target identification and biomarker development Results from clinical trials New: - Preventives - Treatments - Biomarkers - Imaging techniques Laboratory - Bench
Translational Research – State-of-the-Art Translational research offers a holistic approach to cancer management in which laboratory studies are used to optimize the prevention, detection and treatment of cancer, e.g.: • Identification of at-risk individuals and targets for chemoprevention • Development of improved diagnostic and prognostic biomarkers, in particular those where the link to cancer pathology is understood • Discovery and therapeutic exploitation of targets linked to the molecular pathology of cancer • Facilitation of mechanistic early-phase trials of targeted therapies • Evaluation of genomic, proteomic, metabolomic biomarker and molecular imaging methodologies that allow personalised medicine
Translational Research Vision -Cancer Management in 20?? • Genetic analysis at birth to predict life-time risk • Lifestyle advice, and possibly chemoprevention, to minimise risk • Screening using metabolomic, proteomic or genomic techniques, with imaging, to facilitate early detection and accurate diagnosis • If cancer is detected, surgery and/or targeted chemo/radio therapy, with extensive use of prognostic and predictive biomarkers, and imaging technologies, to facilitate curative personalised medicine
Key Objectives in Translational Research • Drug Discovery and Development • Well established in both academic and Pharma/Biotech • Recent advances in cancer biology are providing a rich source of new targets for exploitation • New technologies in cancer drug discovery have the potential to greatly accelerate both drug discovery and development • Biomarker Identification and Qualification • Not historically a strength of Pharma/Biotech • Benefits from strong academic input • Well characterized populations and tissue collections essential • Generally introduced at too late a stage into drug discovery and development • The Holy Grail – Fully integrated biomarker and drug discovery and development
Cancer Research UK and Drug Development Pre-clinical development and early Phase clinical trials The New Agents Committee of Cancer Research UK has taken OVER ONE HUNDRED new cancer treatments into early Phase clinical trials (1980-2007) Later stage clinical trials Cancer Research UK is the major funder of late stage trials and cancer clinical trials units in the UK Interactions with Pharma and Biotech Cancer Research UK has a world-class technology transfer capability in Cancer Research Technology
Past Cancer Research UK Success in Academic Drug Discovery Walter Ross – Chlorambucil Melphalan Busulphan Ken Harrap and Tom Connors – Carboplatin Malcolm Stevens – Temozolomide
Contemporary Drug Discovery Combinatorial chemistry Medicinal chemistry Structure-based design Compound Collections Lead Optimisation In vivo Evaluation Hit-to-lead Development Cellular Mechanism of Action Target ID/validation High-throughput Compound Screening Clinical Evaluation
Patents Animal studies Cell-based assay Absorption, Distribution, Metabolism, Elimination
Targeted Therapies – Science Fact not Science Fiction • Antiendocrine agents • Growth factor and growth factor receptor antagonists • Trastuzumab, cetuximab, gefitinib, erlotonib, lapatinib, sorafinib, sunitinib • Second messenger or signal transduction inhibitors • Imatinib, sorafinib • Regulators of gene expression • All-trans retinoic acid
Single Agent Activity of Targeted Therapies – Objective response rates • Imatinib • CML >90%, Glioma ≤10%, GIST ca. 50% • Trastuzumab • Breast cancer 10-30%, ovary <10% • Gefitinib, Erlotinib • NSLC 10-30%, SCCHN <10% • All-trans retinoic acid • Acute promyelocytic leukaemia >90% • Sunitinib • Renal ca. 40%
Potential Reasons for the Modest Activity of Single Agent Targeted Therapies • Lack of “addiction” to the target – Tumour cells utilise multiple pathways for survival and growth • Genetic instability – Tumour cells rapidly develop drug-insensitivity: target mutation or amplification, up-regulation of alternative pathways or resistance mechanisms • Failure to select potentially sensitive patients for therapy • Inherent pharmacology - Drugs targeted at oncogene products inhibit tumour growth but do not cause tumour regression
Solutions to the Modest Activity of Molecular Therapies • Rational Combination therapy – targeted and/or cytotoxic • “Multi-targeted” targeted agents • Early intervention – chemoprevention • Exploitation of host stromal targets • Patient and population enrichment strategies - Biomarkers • Agents that directly promote cell death
Experimental Cancer Medicine Centre Network • £35 million joint initiative between CR-UK and the Departments of Health in England, Scotland, Northern Ireland and Wales to develop and expand a major network of Centres over 5 years under the auspices of the National Cancer Research Institute • Builds on successful elements of the Departments of Health-funded National Translational Cancer Research Network (NTRAC) • Aims to integrate laboratory and clinical patient-based research to speed up the development of new therapies • Provides funds for infrastructure costs for translational research, knowledge sharing and resources to benefit cancer patients • Underpins translational work to develop new anti-cancer drugs and biomarkers • 19 centres of excellence awarded ECMC status by and international review panel • Funding started April 2007
Expertise in the ECMC Network - I • Belfast – Biomarkers, pharmacokinetics and pharmacodynamics • Birmingham – Immunotherapy, gene therapy and biomarkers • Cambridge – Biomarkers, imaging, informatics and genomics • Cardiff – Pathology, haematology and tissue resources • Edinburgh – Informatics, pharmacokinetics and pharmacodynamics • Glasgow – Pharmacokinetics and pharmacodynamics, gene therapy • Institute of Cancer Research - Biomarkers, imaging, pharmacokinetics and pharmacodynamics • Imperial College London - Imaging, gene therapy, drug resistance • Kings College London – Genomics, imaging, cell and gene therapy
Expertise in the ECMC Network - II • Leeds – Biomarkers, proteomics, pharmacokinetics and pharmacodynamics • Leicester – Chemoprevention and antibody therapeutics • Liverpool – Pharmacokinetics and pharmacodynamics, proteomics • Manchester – Imaging, pharmacokinetics and pharmacodynamics, immunotherapy • Newcastle – Pharmacokinetics and pharmacodynamics, imaging • Oxford – Angiogenesis and immunotherapy • Sheffield – Bone oncology, vascular targeted therapies • Southampton – Immunotherapy • St Bartholomew's and the London School of Medicine – Gene therapy, imaging and biomarkers • University College London – Immunotherapy and antibody targeted therapies, imaging, bioinformatics
Objectives of the ECMC Network • To expand the portfolio of experimental cancer medicine in the UK • To provide a single focus for research charity, industry and the Department of Health's experimental cancer medicine activity • To make the UK an attractive location for industry-sponsored experimental cancer medicine • To provide consumer engagement and involvement in experimental cancer medicine, and to expedite the introduction of new cancer medicines
Development of the ECMC Network - I • Establish a new model: A network for the community based on collaboration and teamwork, a network of membership, no figure heads • Role of ECMC Secretariat: • Support the network in its activities, and facilitate communication and collaboration • Manage and administer the finances of the Network and Secretariat (secretariat budget) • Support specific groups within experimental cancer medicine to develop best practices and standardised shared resources: • ECMC Bio-Analysis and Quality Assurance group • ECMC Research Nurse group • ECMC Data managers group • ECMC Imaging group
Development of the ECMC Network - II • Support for regular ECMC network meetings and ad hoc workshops • Support biannual scientific fora: • Early Clinical Trials Forum – 1st Meeting held December 2006 • Translational Research in Late Phase Trials Forum - 5 July 2007 • Theme: Biomarkers in Late Phase Clinical Trials • Workshops: Genomics and proteomics in sample analysis, bio-banking and tissue resources, biomarkers in development of EGFr/ErbB inhibitors • Make available up-to-date information on open ECMC clinical trials on the CancerHelp UK clinical trials database • Working with consumer groups to promote consumer involvement in the Network • Develop branding/communication strategy • Interface with other relevant committees, industry and external bodies
Conclusions • Translational research offers the prospect of significant advances in patient management • The Experiment Cancer Medicine Centre network provides the framework and infrastructure support for translational cancer research in the UK • The ECMC is a key partnership between government, cancer charities, industry and consumers
Acknowledgements • Dr Mags Sara and Ms Kate Etchells – ECMC Secretariat • National Cancer Research Institute – Dr Jane Cope • Devolved Departments of Health • Colleagues in the ECMC network • CancerHelp UK • Consumers