Download
1 / 41
440 likes | 672 Views
GnRH. What triggers human puberty is one of the central mysteries of reproductive biology. What factors are responsible for the amplification of the pulsatile gonadotrophin-releasing hormone (GnRH) signal intrinsic to GnRH neurones (1) at the expected time of sexual maturation?

E N D
GnRH What triggers human puberty is one of the central mysteries of reproductive biology. What factors are responsible for the amplification of the pulsatile gonadotrophin-releasing hormone (GnRH) signal intrinsic to GnRH neurones (1) at the expected time of sexual maturation? What factors modulate the amplitude and frequency of GnRH throughout reproductive life, particularly during the female menstrual cycle?
GnRH L’ormone che induce il rilascio delle gonadotropine (GnRH) è il principale regolatore della cascata ormonale coivolta nella riproduzione ed è stato isolato dall’area preottica dell’ ipotalamo di mammiferi. E’ un decapeptide ed è rilasciato nel circolo sanguigno a livello della eminenza mediana in modo pulsatile di quantità precise dagli assoni di neuroni i cui terminali sono localizzati nell’ipofisi anteriore. Il rilascio di questo ormone avviene ogni 30-120 minuti il quale regola la biosintesi e la liberazione di LH e FSH dall’ipofisi anteriore. La frequenza di rilascio del GnRH è massima durante l’ovulazione mentre è ridotta al minimo durante la fase luteale. La secrezione di GnRH e’ controllata negativamente da steroidi gonadici mentre neurotrasmettitori ad azione inibitoria quali il GABA, aminoacidi eccitatori (acido glutammico), peptidi oppioidi endogeni, monoamine del sistema noradrenergico, dopaminergico e serotoninergico, acetilcolina, melatonina, ossitocina modulano il rilascio di GnRH.
GnRH deficiency The syndrome characterised by endogenous GnRH deficiency, i.e. normosmic idiopathic hypogonadotrophic hypogonadism (nIHH) is characterised by abnormal/absent GnRHinduced luteinising hormone (LH) pulsations in which patients present with delayed or absent pubertal development and other associated somatic abnormalities. Although rare, nIHH is a disease caused by defects in the synthesis, secretion and action of GnRH and, therefore, has long been considered an important entrée to understanding the modulators of GnRH in humans.
Sequenza di eventi causati dal GnRH: 1) Induce secrezione di FSH ed LH che a loro volta stimolano l’accrescimento di follicoli ovarici e la produzione di testosterone o estradiolo
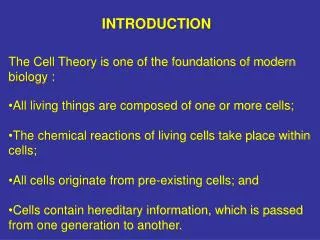
Kisspeptin released by neurons in the AVPV and Arc stimulates GnRH release, which induces the release of LH and FSH.
REVIEW ARTICLE published: 09 April 2012 Estrogen has a bimodal effect on the hypothalamus with both an inhibitory and stimulatory influence on GnRH secretion. The stimulatory effect of estrogen is seen at the end of the follicular phase where estrogen triggers the preovulatory GnRH surge. The inhibitory effect of estrogen on GnRH secretion and GnRH gene expression has been shown in in vivo studies in several mammalian species. Studies in ewes indicate that estrogen inhibits GnRH pulse amplitude in the early follicular and luteal phase of the cycle. The more prevalent hypothesis is that the influence of estrogen on GnRH is not direct but is conveyed to GnRH neurons via presynaptic afferents from adjacent cells that express ER (now thought to be kiss1 neurons).
Kisspeptin Kisspeptin peptides are the most powerful stimulators of gonadotrophin secretion that have ever been studied in mammalian species, including rodents on a molar basis (19–24), sheep (25) and monkeys (26). Intracerebral doses as low as 1 fmol evoke significant LH responses (20). The effects of kisspeptin on LH can be completely abrogated by the co-administration of a GnRH antagonist, demonstrating that this protein is acting through the GnRH receptor to stimulate LH release (i.e. hypothalamic effect) (20). Kisspeptin is unable to stimulate LH release when given to GPR54 knockout mice, suggesting that the stimulatory effects of this peptide are mediated only through its cognate receptor
Kisspeptins and KISS1R Discovery and nomenclature Kisspeptins comprise a family of peptides derived from the primary translation product of the KISS1 gene, localized to chromosome 1, which were identified more than a decade ago (Lee et al. 1996). These peptides were discovered as the result of a systematic bioinformatics search for processed peptides encoded by the human genome (Ohtaki et al. 2001), and simultaneously by the isolation of a biological activity from human placenta and its identification by mass spectrometry (Kotani et al. 2001). Proteolytic processing of the full-length 145 amino acid kisspeptin protein results in shorter fragments of the carboxyl (C)-terminus region of the molecule with 54 (KP-54; previously designated metastin), 14 (KP14), 13 (KP-13) or 10 (KP-10) amino acids (Kotani et al. 2001, Ohtaki et al. 2001). Initially, the largest cleavage product, KP-54 was identified for its ability to suppress the metastatic potential of malignant melanoma cells (Lee et al. 1996, Lee & Welch 1997) and it was therefore termed ‘metastin’ (Ohtaki et al. 2001). Interestingly, the naming of the gene KISS1 and its product, kisspeptin (aka metastin), was made by the team of scientists who discovered the gene in the town of Hershey, Pennsylvania, famous for its chocolate ‘kisses’, with inclusion of the terminology ‘SS’ also indicating a suppressor sequence. The term ‘kisspeptins’is now widely employed to collectively describe this family of peptides that show an Arg–Phe–NH2 motif at the C-terminus, characteristic of the extensive RF-amide peptide superfamily (Roa et al. 2008).
GnIH possesses the RFamide (Arg-Phe-NH2) motif at its C-terminus and thus belongs to the RFamide peptide family. The first identified RFamide peptide, Phe-Met-Arg-Phe-NH2 (FMRFamide), was a cardioexcitatory molecule isolated from the ganglia of the venus clam Macrocallista nimbosa (35). In 2000, an RFamide peptide was isolated from the brain of the Japanese quail using high-performance liquid chromatography (HPLC) and a competitive enzyme-linked immunosorbent assay for the dipeptide Arg-Phe-NH2 (8). The isolated peptide was a previously-unreported dodecapeptide (SIKPSAYLPLRFamide). The cDNAs of human, monkey and cow (bovine) also encoded three GnIH orthologs, which were termed RFRP-1, -2 and -3 (62). However, in contrast to other vertebrates, RFRP-2 is not predicted to be an RFamide peptide, although this mature peptide has not yet been isolated so it is unknown if it is actually cleaved from the precursor.
The HeLa cell line was derived from cervical cancer cells of Henrietta Lacks, a patient who died of her cancer on October 4, 1951. Arr = Arrestina extracellular-signal-regulated kinases (ERKs)
Low levels of GnRH release during the wake period in early puberty are thought to be dependent on negative feedback from progesterone (P4), consistent with a sharp rise in circulating P4 levels in the morning. P4 inhibition of GnRH neuronal activity occurred when both excitatory inputs were blocked, supporting the hypothesis that P4 can act directly on GnRH neurons.
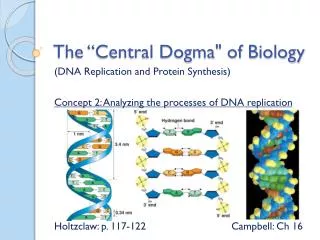
GnRH analogs pharmacological physiological GnRH agonist FSH & LH Pulsatile GnRH GnRH FSH LH GnRH antagonist FSH & LH FSH & LH
It took a considerable period of time after the elucidation of GnRH to generate clinically useful antagonists (GnRH ant). The third generation compounds (Ganirelix (Organon, Cambridge, UK) and Cetrorelix (Merck-Serono, Feltham,UK)) reached the market in 2001.Their ability to induce immediate suppression and subsequent rapid recovery of pituitary function is particularly appropriate to their short term use in IVF.
There are, however, differences between the GnRHa induced LH surge and the LH surge of the natural cycle; the LH surge of the natural cycle being characterized by three phases with a total duration of 48 h (Hoff et al., 1983) as compared with the GnRHa induced LH surge consisting of two phases with a duration of 24–36 h (Itskovitz et al., 1991). This leads to a significantly reduced total amount of gonadotrophins (LH and FSH) released from the pituitary when GnRHa is used to trigger final oocyte maturation (Gonen et al., 1990; Itskovitz et al., 1991) resulting in corpus luteum deficiency and a defective luteal phase (Segal and Casper, 1992; Balasch et al., 1995).
DEGARELIX Degarelix is a synthetically modified analogue of azaline B with GnRH antagonist activity. It was approved by the US FDA in December 2008 for the management of advanced prostate cancer.
“Early studies in the structure–activity relationships of GnRH peptides identified His2 as critical for receptor activation.”
Curr Opin Obstet Gynecol. 2010 Aug;22(4):283-8. Gonadotropin-releasing hormone agonist and add-back therapy: what do the data show? Surrey ES. Colorado Center for Reproductive Medicine, Lone Tree, Colorado, USA. Abstract PURPOSE OF REVIEW: Endometriosis is a gynecologic disorder that can lead to debilitating chronic pelvic pain and infertility. Gonadotropin-releasing hormone agonists (GnRHa) have emerged as a primary medical therapy for patients with symptomatic disease,but secondary hypoestrogenic side effects may limit compliance. Add-back therapy is a means of surmounting this problem. RECENT FINDINGS: Progestins such as norethindrone acetate may be administered with or without addition of low doses of estrogens to safely and effectively extend GnRHa therapy while minimizing side effects. Recent studies have demonstrated that the use of add-back enhances compliance and duration of therapy. The initiation of an add-back should not be deferred given evidence demonstrating an increase in vasomotor symptoms and bone loss if not administered concomitantly. The subset of adolescents with endometriosis who require GnRHa therapy should be administered an add-back, but require careful monitoring of bone mineral density. SUMMARY: Implementation of an appropriately selected add-back will significantly reduce hypoestrogenic side effects, enhance compliance, and allow for prolongation of therapy without interfering with the efficacy of GnRHa in treating symptomatic endometriosis.
BackgroundSystematic reviews have found that luteinizing hormone – releasing hormone (LHRH) agonists are effectivein treating premenopausal women with early breast cancer. Methods We conducted long-term follow-up (median 12 years) of 2706 women in the Zoladex In premenopausal Patients (ZIPP), which evaluated the LHRH agonist goserelin (3.6 mg injection every 4 weeks) and tamoxifen (20 or 40 mg daily), given for 2 years. Women were randomly assigned to receive each therapy alone, both, or neither, after primary therapy (surgery with or without radiotherapy/chemotherapy). Hazard ratios and absolute risk differences were used to assess the effect of goserelin treatment on event-free survival (breast cancer recurrence, new tumor or death), overall survival, risk of recurrence of breast cancer, and risk of dying from breast cancer, in the presence or absence of tamoxifen. ResultsFifteen years after the initiation of treatment, for every 100 women not given tamoxifen, there were 13.9 (95% confidence interval [CI] = 17.5 to 19.4) fewer events among those who were treated with goserelin compared with those who were not treated with goserelin. However, among women who did take tamoxifen, there were 2.8 fewer events (95% CI = 7.7 fewer to 2.0 more) per 100 women treated with goserelin compared with those not treated with goserelin. The risk of dying from breast cancer was also reduced at 15 years: For every 100 women given goserelin, the number of breast cancer deaths was lower by 2.6 (95% CI = 6.6 fewer to 2.1 more) and 8.5 (95% CI = 2.2 to 13.7) in those who did and did not take tamoxifen, respectively, although in the former group the difference was not statistically significant. ConclusionsTwo years of goserelin treatment was as effective as 2 years of tamoxifen treatment 15 years after starting therapy. In women who did not take tamoxifen, there was a large benefit of goserelin treatment on survival and recurrence, and in women who did take tamoxifen, there was a marginal potential benefit on these outcomes when goserelin was added.
Background: The usefulness of long-term, low-dose gonadotropin-releasing hormone agonist (GnRHa; buserelin acetate) therapy, so-called draw-back therapy, for the treatment of adenomyosis was investigated . Material/Methods: A retrospective observational study was conducted covering the period between January 2003 and March 2008. The subjects consisted of 12 patients with adenomyosis who underwent draw-back therapy for 2 years and had previously received GnRHa. GnRHa was initiated at 900 μg/day (6 nasal sprays/day). When the CA-125 level normalized, the GnRHa dosage was adjusted to 150–750 μg/day to achieve a plasma estradiol (E2) concentration of 20–50 pg/ml (i.e., the therapeutic window). Pain during withdrawal bleeding and chronic pelvic pain were assessed using a visual analogue scale. In addition, bone mineral density (BMD) of the lumbar vertebrae was measured using dualenergy X-ray absorptiometry. Results: The mean GnRHa dose during draw-back therapy was 435 μg/day (2.9 nasal sprays/day). The mean E2 level during draw-back therapy was 36.3±14.3 pg/ml. The intensity of chronic pelvic pain was signifi cantly lower during draw-back therapy than before draw-back therapy, and was nearly eliminated in many patients (4.8±1.2 vs. 0.6±0.7, respectively [p=0.000]). Compared to the severity of vasomotor symptoms during previous regular GnRHa therapy, the severity of vasomotor symptoms during draw-back therapy was signifi cantly lower (3.8±0.7 vs 1.1±0.7, respectively [p=0.000]). The decrease in BMD during a 6-month course of treatment was 0.96±0.9%. Conclusions: GnRHa draw-back therapy allowed maintenance of plasma E2 levels within the therapeutic window. GnRHa can thus be administered for long periods of time while maintaining therapeutic effects on adenomyosis and suppressing adverse events.
In this study, we aim to evaluate the clinical outcome and patient’s convenience of single administration of long-acting GnRHa (goserelin depot) as compared with multiple daily administrations of short-acting GnRHa (buserelin or leuprorelin).
With its extreme molecular weights, hCG is the longest circulating molecule in human blood with a circulating half life of 36 hours. Secondly, as described in this review, there are amazingly 5 unique variants of hCG, each having identical amino acid sequence, produced by different cells and having independent functions. These are hCG, sulfated hCG, hyperglycosylated hCG, hCG free ß-subunit and hyperglycosylated hCG free ß-subunit. There is no other molecule like hCG. A major function of hCG during pregnancy can be described as driving hemochorial placentation, or the efficient method whereby humans drive nutrient transfer to the fetus.
The alfa-subunit of hCG comprises 92 amino acids and 2 N-linked (Asn-linked) oligosaccharides [46]. The ß-subunit comprises 145 amino acids, 2 N-linked (Asn-linked) and 4 O-linked (Ser-linked) oligosaccharides [46].
hCGs in pharmacological preparations were originally derived from urinary samples of pregnant women. Urinary hCG (uhCG) products may have, however, great biological variability with a significant batch-to-batch variation due to their human origin. Therefore, recombinant technology has been introduced for the production of recombinant hCG (rhCG) with high-purity and batch-to-batch consistency. Other advantage of rhCG products over uhCG preparation is their availability in different dose strengths that provide an opportunity for individualized therapy.
Human chorionic gonadotrophin (hCG) has been the gold standard for ovulation induction as a surrogate for the mid-cycle LH surge for several decades. Due to structural and biological similarities, hCG and LH bind to and activate the same receptor, the LH/hCG receptor (Kessler et al., 1979). An important difference, however, exists between the half-life of LH and hCG, as the half-life of LH is 60 min (Yen et al., 1968) whereas that of hCG is >24 h (Damewood et al., 1989). Due to its prolonged circulatory half-life, hCG exerts a sustained luteotropic activity, and may induce the occurrence of ovarian hyperstimulation syndrome (OHSS) (Delvigne and Rozenberg, 2002). When GnRH antagonist protocols were introduced for the prevention of a premature LH surge (Albano et al., 1997; Itskovitz-Eldor et al., 1998; Borm and Mannaerts, 2000) it became possible to trigger final oocyte maturation and ovulation with a single bolus of a GnRH agonist (GnRHa) as an alternative to hCG (Nakano et al., 1973).
In both rodents (4) and humans (10), AMH expression starts in the columnar granulosa cells of primary follicles, is highest in granulosa cells of preantral and small antral follicles, and gradually diminishes in the subsequent stages of follicle development so that AMH is no longer expressed during the gonadotropin-dependent terminal stages of follicle development. In addition, AMH expression disappears when follicles become atretic.