Download
1 / 12
130 likes | 318 Views
Development and description of new criteria for the endoscopic diagnosis and grading of Barrett’s Esophagus. Prateek Sharma, M.D. Kansas City, USA Chairman of the Barrett’s Oesophagus Working Subgroup of the International Working Group for the Classification of Oesophagitis. Other Members:

E N D
Development and description of new criteria for the endoscopic diagnosis and grading of Barrett’s Esophagus Prateek Sharma, M.D.Kansas City, USAChairman of the Barrett’s Oesophagus Working Subgroup of the International Working Group for the Classification of Oesophagitis
Other Members: – D. Armstrong – J. Bergman – J. Dent – L. Gossner – M. Hongo – Y. Hoshihara – J. Jankowski – O. Junghard – R. Kiesslich – L. Lundell – G. Tytgat – M. Vieth – L. Yerian Members of the Barrett’s Oesophagus Working Subgroup at December 2006 Chair: P. Sharma
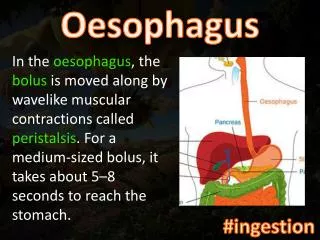
Diagnosis of Barrett’s Esophagus Endoscopic recognition of Barrett’s Esophagus requires … • Recognition of endoscopic landmarks: gastro-esophageal junction, squamo-columnar junction, diaphragmatic hiatus • Presence of a columnar lined esophagus (i.e. esophageal columnar metaplasia)
Endoscopic recognition of Barrett’s Esophagus Columnar lined esophagus
Endoscopic grading of Barrett’s Esophagus • Terminology issues • Recognition of endoscopic landmarks • Essential features for a new classification • Testing new criteria
Barrett’s Oesophagus Working Subgroup – Primary Aim • Endoscopic diagnosis and grading of the extent of Barrett’s Esophagus: • Consensus-based development of criteria • Inter- and intra- observer variation studies • Consensus-based re-evaluation of criteria • Development of explicit criteria for diagnosis and grading of extent of Barrett’s Esophagus
Barrett’s Oesophagus Working Subgroup – Issues to be addressed What are the distinctive landmarks required for endoscopic diagnosis for Barrett’s Esophagus? What practical robust criteria can we develop to ensure that observers recognize these landmarks reliably? What criteria best describe the length of Barrett’s Esophagus in individual patients?
Top of fold Top of fold The major endoscopic landmark for the gastro-esophageal junctionThe top of the gastric mucosal folds
16 M:Maximum extent = 14cm 14 12 Distance in cm from gastro- esophageal junction 10 8 C:Circumferential extent = 6cm 6 4 Correctly identify gastro-esophageal junction 2 0 Recognize hiatus hernia The Prague Barrett’s C&M Criteria
Endoscopic grading of Barrett’s Esophagus The Prague Barrett’s C&M Criteria • Practical and user friendly • Based on – Circumferential and Maximum extent • For a patient who has 4 cm of circumferential metaplasia and a 2 cm tongue above this, as in the endoscopic photograph that follows:Prague; C4 & M6
C4 M6
Diagnosis of Barrett’s Esophagus • Further characterization of Barrett’s Esophagus requires multiple biopsies from the columnar lined segment to document metaplastic and dysplastic epithelium • The Prague Barrett’s C&M Criteria • alert the endoscopist to the presence of a columnar lined esophagus • grade the Circumferential and Maximal extent of the columnar lined esophagus