Download
1 / 40
400 likes | 694 Views
III YEARS BLOCK 8 – OESOPHAGUS SYMPOSIUM OBJECTIVES. • Recognition of common diseases of the oesophagus. Cancer and reflux • Principal manifestations of oesophagus disease • Dysphagia • Heartburn • Odynophagia • Haemorrhage • Principles of diagnosis and treatment. THE SYMPOSIUM.

E N D
III YEARS BLOCK 8 – OESOPHAGUS SYMPOSIUMOBJECTIVES • Recognition of common diseases of the oesophagus. Cancer and reflux • Principal manifestations of oesophagus disease • Dysphagia • Heartburn • Odynophagia • Haemorrhage • Principles of diagnosis and treatment
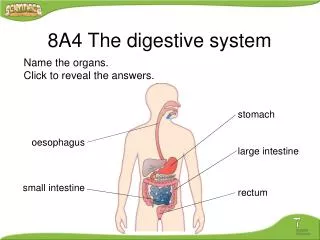
THE SYMPOSIUM Applied Anatomy • Topographic anatomy - neck - mediastinum - abdomen • Organisation of muscles • The sphincter apparatus • Nerve Supply • Blood supply • Histology
Applied Physiology Mechanism of swallowing Sphincter mechanism
Pathology Degenerative and structural diseases • Diverticula • Fistulae (and sinuses) • Stenotic lesions including atresia • Tears (Mallory-Weiss) or Perforations (Boerhaave)
Neoplastic Diseases • Benign (rare) • Malignant - squamous cell - adenocarcinoma Myoneural • Achalasia • Nutcracker oesophagus • pseudo bulbar palsy
MYONEURAL DISORDERS Achalasia Nutcracker oesophagus Pseudo bulbar palsy
Inflammatory diseases • Infective:- Candidiasis esp with HIV TB Other • Collagen vascular disorders Scleroderma • Chemical injury external acid/alkali ingestion acid/alkali reflux
Pathophysiology Effects of fistulae – pulmonary aspiration Effects of reflux – oesophagitis and fibrotic stricture Effects of strictures – dysphagia Barretts Disease – premalignant Varicose veins (varices) - haemorrhage
Cardinal Symptoms and Signs • Dysphagia • Heartburn and odynophagia • Haematemesis/melaena • Choking • Regurgitation/vomitting • Nutritional status
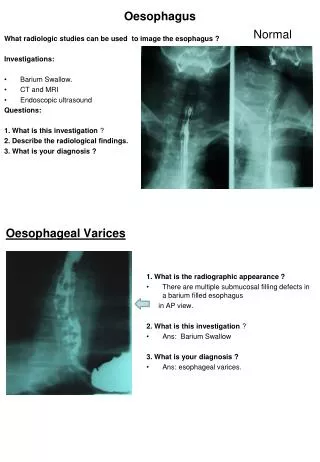
SPECIAL DIAGNOSTIC INVESTIGATIONS Plain Radiograph especially for foreign body Radiographic Oesophagogram Videofluoroscopy Endoscopy Biopsy - cytology - histology Manometry Ambullatory pH metre
PRINCIPLES OF TREATMENT Reflux Oesophagitis • Medical • Surgical - conventional - minimal access (endoscopic)
HAEMORRHAGIC VARICES • Medical - β-blockers, somatostatin • Mechanical – balloon tamponade • Endoscopic - sclerosis - banding Surgical - oesophageal transaction -gastric devascularisation -portosystemic shunt incl TIPS
CARCINOMA Curative treatment • surgical • radiation • chemotherapy • combination
PALLIATIVE TREATMENT • Surgical • Radiation • Chemotherapy • Endoluminal intubation • Dilatation • other
ACHALASIA Surgical – myotomy Dilatation Medical – Ca++ channel blockers, vaso- dilations Botulisation
BARRETT’S OESOPHAGUS PREMALIGNANT • Treat Reflux • Mucosectomy • Oesophagectomy
ADDITIONAL READING • Oxford Textbook of Surgery P J Morris and R A Malt • Textbook of Oesophageal Disease de Meester
Oesophagus Case Study PROBLEM OF DYSPHAGIA
History • Progressive dysphagia. • Dysphagia for solids x 2 months. • Odynophagia – retrosternal. • Severe weight loss – 15 kg in 3 months. • No history of • Heartburn • Symptoms not related to recumbency
Systemic & Social History • Type II diabetic x 6 years. On Glucophage & Diamicron. • HT x 4 years. On Coversyl. • Non – smoker. Minimal alcohol intake.
Clinical examination • Chronically ill, wasted 62 year old male. • Systemic examination normal.
Differential diagnosis • CA OESOPHAGUS • CA STOMACH • CHRONIC PEPTIC ULCER OESOPH • OESOPHAGITIS-?candidiasis/HIV • Achalasia
Investigations What Order of Diagnostic Investigation
Oesophagoscopy • Mild distal oesophagitis with Candidiasis • Tight oesophageal stricture at oesophago-gastric junction. Clinically benign. • Stricture easily dilated to 15 mm. • 5 cm hiatus hernia. • Multiple biopsies taken.
Blood Tests • HIV negative • Serum Albumin 14 • Serum Glucose 5.4
Biopsy Result • Fibrosis with signs of chronic inflammation in distal oesophagus. • No sign of malignancy. • No columnar metaplasia in distal esophagus.
Differential diagnosis • Oesophageal cancer • Complicated Gastro-Esophageal Reflux Disease (GERD) • Candidiasis
Clinical Course • Admission • Treatment • High protein diet. • Oral diabetic • Anti-hypertensives • PPI • Repeat oesophagoscopy & biopsies: same as before, benign. • 24 hour pH-metry & oesophageal manometry: Normal but on PPI.
Clinical Course • Improved & gained weight on the ward. • Discharged on PPI & Fluconazole for review in one month.
Clinical Course • The patient was followed up after one month. • Symptoms had recurred: • Progressive dysphagia. • Weight loss. • Repeat oesophagoscopy, dilatation & biopsy: No change. • Sent home on PPI
Clinical Course • Patient was readmitted after one month – symptoms had again recurred. • Fourth oesophagoscopy + biopsies + dilatation was performed. • A repeat 24 hour pH-metry & manometry was booked, this time PPI was stopped one week prior to test: Normal