Download
1 / 23
440 likes | 1.56k Views
Necrotizing Enterocolitis. Presented by Dr Akram Sa’ade Moderator: Dr Yousef Abu Osba. History. Ahmed is a newborn male baby , a product of caesarean section at 27 week gestational age due to antepartum hemorrhage on 28 July 2003 in a major hospital in Amman.

E N D
Necrotizing Enterocolitis Presented byDr Akram Sa’ade Moderator: Dr Yousef Abu Osba
History • Ahmed is a newborn male baby , a product of caesarean section at 27 week gestational age due to antepartum hemorrhage on 28 July 2003 in a major hospital in Amman.
Cource in the referral hospital • The baby was immediately admitted and treated as a case of • -Respiratory Distress Syndrome. • -Suspected Sepsis.
Course in the referral hospital • Put on mechanical ventilator. • Covered by Ampicillin and ceftazidime. • Given Pentaglobin. • Received 3 doses of surfactant. • Received packed RBCs and plasma many times.
Course in the referral hospital • Feeding started at the age of 10 days ;but 2 days later the baby noticed to have abdominal distention;followed by bluish discoloration of the skin overlying the abdomen and scrotum. • Feeding stopped. • Metronidazole added.
The baby referred to our NICU At the age of 3 weeks as a case of • Prematurity. • Respiratory Distress Syndrome. • Cholestatic Jaundice. • Suspected Retroperitonial Hemorrhage. • Suspected IntraventricularHemorrhage.
Course in our NICU • The baby continued on mechanical ventilator with the following setup RR 15 PiP 12 FiO2 100 PEEP 3 with gradual weaning according to the respiratory status.
Examination • Vital signs HR 140 bpm RR 40/min BP 75/39mmHg Temp 35.9 C
Examination Head and Neck • Pale. • No dysmorphic features. • No cyanosis. • Normal neck examination.
Examination Chest • No deformities. • Good air entry bilaterally. • Normal vesicular breathing. • No added sounds.
Examination Cardiovascular • Normal 1st and 2nd heart sounds. • No murmurs. • Intact peripheral pulses.
Examination Abdomen • Distention, abdominal girth=23cm. • Bluish discoloration of the skin overlying • the abdomen. • Palpated mass about 2cm in diameter • just below the left costal margin. • Bilateral inguinal hernia. • Scrotal swelling with bluish discoloration • of the overlying skin.
Investigation • WBC=14.9 x 10 9 ; N=65 % L=25% PCV=36% ;PLT=75x10 9 • Na=132 meq/l ;K=4 meq/l • Ca=8.5 mg/dl ;CRP=48 • TSB=8.1mg/dl ; Direct bilirubin=3.5mg/dl • ABGs pH=7.45 PaO2=186 PaCO2=36 HCO3=24
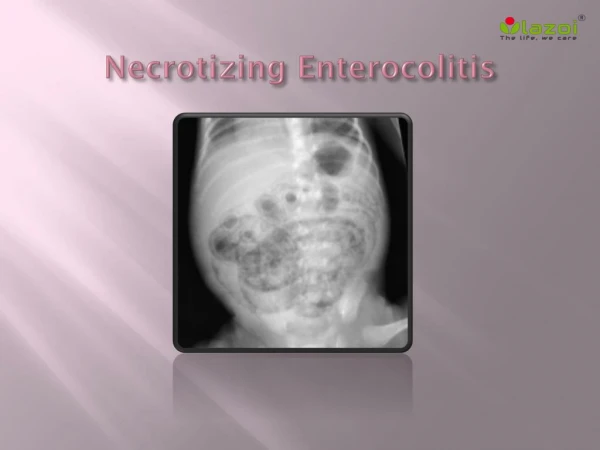
Imaging • Chest X-Ray Resolving respiratory distress syndrome. • Abdominal Ultrasound Bilateral hydronephrosis ,Fluid collection. • Head Ultrasound No hemorrhage. Chest
Management • NPO and NGT free drainage. • Central line. • IVF[that was changed according to blood glucose and electrlytes . • Packed RBCs and Plasma. • Metronidazole,Imipinem and Teicoplanin. • Pentaglobin. • Vitamin k.
Necrotizing Enterocolitis suspected and abdominal erect and supine X-rays done and revealed: Multiple air fluid levels with air under the diaphragm ,which suggested a perforated hollow viscus.
Pediatric surgeon consultation • Peritoneal drainage performed, the drained peritoneal fluid was bloody, dirty and under pressure initially about 50cc. • Peritoneal lavage done with Cefotaxime and saline.
Drain removed 5days later after clearing and decreasing in amount of the discharge. • Follow up X-Rays revealed ---no air fluid levels -disappearance of air under the diaphragm.
Course in the hospital • 10 days after admission Abdominal Ultrasound repeated and revealed : • disappearance of fluid collection. • improvement of hydronephrosis.
Course in the hospital • 2 weeks after admission -The general condition was significantly improved but unfortunately the condition deteriorated with development of metabolic and respiratory acidosis for which sepsis workup done that were all negative apart from growth of klebsiella from the ETT. • Imipinem and Teicoplanin discontinued. • Ceftazidime and Amikacin started. • Fluconazole added. • Pentaglobin given.
Course in the hospital • In the last 3 days The patient developed cardiopulmonary compromise for which : *Dopamine and Dobutamine and NaHCO3 continuous infusion started . but the baby continued to have bradycardia and metabolic acidosis.
Course in the hospital • Inspite of continuous intensive management ,the condition deteriorated and the patient resuscitated for 3 times • Died on 3 AUGUST 2003.
Final Diagnosis • Prematurity. • Respiratory Distress Syndrome. • Necrotizing Enterocolitis. • Cholestatic Jaundice.