Download
1 / 20
570 likes | 2.05k Views
Necrotizing Enterocolitis. By Dr. Nahed Al- Nagger. Learning Objectives:. Define Necrotizing Enterocolitis. Mention factors lead to development of NEC. Describe the incidence of NEC. List the causes of NEC. Determine the manifestations of NEC. State how to diagnose NEC.

E N D
Necrotizing Enterocolitis By Dr. Nahed Al- Nagger
Learning Objectives: • Define Necrotizing Enterocolitis. • Mention factors lead to development of NEC. • Describe the incidence of NEC. • List the causes of NEC. • Determine the manifestations of NEC. • State how to diagnose NEC. • Discuss the management of NEC.
Necrotizing Enterocolitis " Necrotizing " Death or necrosis of tissue, "entero" Small intestine, "colo" Large intestine. "itis" Inflammation.
Necrotizing Enterocolitis Definition: A gastrointestinal disease that mostly affects premature infants. NEC is an acute inflammatory disease the bowel (intestine) or part of the bowel. NEC is the most common and serious gastrointestinal disorder among hospitalized preterm infants.
Predisposing Factors of NEC: Intestinal ischemia. Colonization by pathogenic bacteria. Formula feeding.
Incidence of NEC: • Occurs within the first 2 weeks of life, usually after milk feeding has begun. • About 10% of babies weighing less than 1,500 grams experience NEC.
Causes of NEC • The exact cause of NEC is unknown. But several theories exist. • The intestinal tissues of premature infants are weakened by too little oxygen or blood flow, • and when feedings are started, the added stress of food moving through the intestine allows bacteria that are normally found in the intestine to invade and damage the wall of the intestinal tissues. • The damage may affect only a short segment of the intestine, or it may progress quickly to involve a much larger portion.
Causes of NEC • The infant is unable to continue feedings and starts to appear ill if bacteria continues to spread through the wall of the intestines and sometimes into the bloodstream. • He may also develop imbalances in the minerals in the blood. In severe cases of NEC, a hole (perforation) may develop in the intestine, allowing bacteria to leak into the abdomen and causing life-threatening infection (peritonitis). • Because the infant's body systems are immature, even with quick treatment for NEC there may be serious complications.
Symptoms of NEC • Abdominal distention. • Bloody stools. • Poor feeding, or feeding intolerance. • Bile-colored (green) vomiting or gastric drainage. • Signs of infection such as lethargy and apnea (cessation of breathing). • Temperature instability.
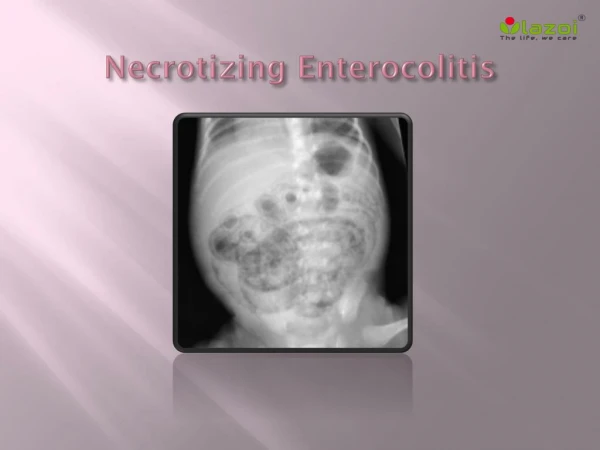
Diagnosis • Abdominal X-ray. • An X-ray may show multiple small bubbles in the wall of the intestine. • In severe cases, the X-ray may reveal air or gas in the large veins of the liver. This air is produced by bacteria in the wall of the bowel. • Organism are often cultured from blood.
Medical Treatment • Stopping all regular feedings. The baby receives nutrients through an intravenous (IV) catheter. • Placement of a nasogastric tube The tube suctions air and fluids from the baby's stomach and intestine, relieving swelling and discomfort. • Starting antibiotic therapy. • Checking stools for blood.
Medical Treatment • If abdominal swelling interferes with breathing, providing oxygen or mechanically assisted breathing. • In severe cases, platelet and red blood cell transfusion may be necessary.
Surgical Treatment A pediatric surgeon examines the intestine and removes only the destroyed parts, leaving as much intestine as possible so that less damaged segments have an opportunity to regain function. In some cases, a drain is placed in the abdomen to remove the infected fluid.
Nursing Intervention • Be aware of the possibility of this disease and infants who are at high risk for developing NEC. • When disease is suspected, assists with diagnostic procedures and implements the therapeutic regimen. • Vital signs, including blood pressure, are monitored for the changes that might indicate bowel perforation, Septicemia.
Nursing Intervention • Measures are instituted to prevent possible transmission to other infants. • Avoid rectal T. because of the increased danger of perforation. • Infants are often left undiapered and positioned supine or on the side to facilitate continuous observation.
Careful attention to nutritional and hydration needs is essential. • Antibiotics are administered as prescribed. • The time at which oral feedings are reinstituted varies considerably but is usually at least 7 to 10 days after diagnosis and treatment . • Feeding is usually re-established using human milk ,if available.
Strict hand washing is the primary barrier to spread, and confirmed multiple cases are isolated. • Persons with symptoms of a GIT disorder should not care for these or any other infants. • Caring with infants after surgery if needed.