Download
1 / 21
230 likes | 883 Views
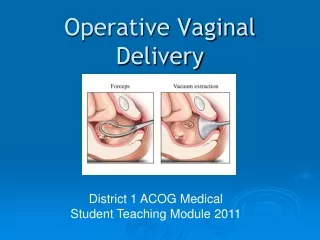
Operative Vaginal Delivery. Normal Birth Mechanism. Introduction. US incidence of Operative Vaginal Delivery (OVD) – 4.5%* Overall rate of OVD declining, but the proportion of vacuum deliveries is 4-times the rate of forceps Forceps deliveries = 0.8% of vaginal births

E N D
Introduction • US incidence of Operative Vaginal Delivery (OVD) – 4.5%* • Overall rate of OVD declining, but the proportion of vacuum deliveries is 4-times the rate of forceps • Forceps deliveries = 0.8% of vaginal births • Vacuum deliveries = 3.7% of vaginal births UpToDate: September 2010
Indications for OVD No indication is absolute • Prolonged 2nd stage • Nulliparous: lack of continuous progress • >3hrs with regional anesthesia • >2hrs w/o regional anesthesia • Multiparous: lack of continuous progress • >2hrs with regional anesthesia • >1hr w/o regional anesthesia • Fetal compromise • Maternal benefit to shortened 2nd stage
Station • At the 0 station, the fetal head is at the bony ischial spines and fills the maternal sacrum. • Positions above the ischial spines are referred to as -1 through -5 • As the head descends past the ischial spines, the stations are referred to as +1 through +5 (head visible at the introitus).
Fetal attitude & lateral flexion of the fetal head A: Synclitism—The plane of the biparietal diameter is parallel to the plane of the inlet B: Asynclitism—Lateralflexion of the fetal head leads to anterior parietal or posterior parietal presentation.
Prerequisites for OVD • Informed consent • Vertex • Engaged • ≥34 weeks (vacuum delivery) • Fully dilated • Membranes ruptured • Adequate maternal pelvis • Adequate anesthesia • Maternal empty bladder • Backup plan • Ongoing fetal and maternal assessment
Contraindication-OVD • Non-cephalic, face or brow presentation • Unengaged vertex • Incompletely dilated cervix • Clinical evidence of CPD • < 34 weeks gestation (vacuum) • Need for device rotation (vacuum) • Deflexed attitude of fetal head • Fetal conditions (e.g. thrombocytopenia)
Classification of OVD • Outlet • Scalp visible @ introitus w/o separating labia • Fetal skull @ pelvic floor • Saggital suture in AP plane (or ROA/LOA) • Fetal head at or on perineum • Rotation < 45 degrees • Low • Leading point of fetal skull > or = +2 station • Rotation < 45 degrees • Rotation > 45 degrees • Mid • Station above +2 station but the head is engaged • High • Not included in classification
Vacuum versus Forceps *ACOG Practice Bulletin #17 (June 2000) **Johnson RB. The Cochrane Library Issue 4, 1999 • “Selection of the appropriate instrument and decisions about the maternal and fetal consequences should be based onclinical findings at the time of delivery.” • A meta-analysis comparing vacuum extraction to forceps delivery showed that vacuum extraction was associated with significantly: • Less maternal trauma • Less need for general and regional anesthesia
Effect of Delivery on Neonatal InjuryTowner D et al. Effect of Mode of Delivery in Nulliparous Women on Neonatal Intracranial Injury. NEJM 1999;341:1709 ICH – Intracranial Hemorrhage