Download

1 / 45
450 likes | 467 Views
Understand the care needed post-lower segment caesarean section (CS). Learn about uterine and vaginal healing, proper nutrition for recovery, perineal pain management, and factors affecting healing. Discover when medical intervention is required.

E N D
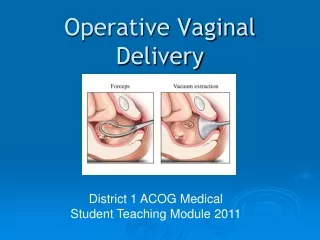
A lower segment caesarean section (CS) will have involved cutting of the major abdominal muscles and damage to other soft tissues. Palpation of the abdomen is therefore likely to be very painful for the woman in the first few days after the operation. The woman who has undergone a CS will have a very different level of physical activity from the woman who has had a vaginal birth. It may be some hours after the operation until the woman feels able to sit up or move about. Blood and debris will have been slowly released from the uterus during this time and, when the woman begins to move, this will be expelled through the vagina and may appear as a substantial fresh-looking red loss.
it is usual for the amount of vaginal loss to lessen and for further fresh loss to be minimal. • All this can be observed without actually palpating the uterus. • After 3 or 4 days an operative birth,abdominal palpation to assess uterine involution can be undertaken by the midwife where this appears to be clinically appropriate. • By this time, the uterus or area around the uterus should not be overly painful on palpation.
where the vaginal bleeding is heavier than expected, the uterine fundus can be gently palpated. • If the uterus is not well contracted then medical intervention is needed. • Uterine stimulants (uterotonics) of an intravenous infusion of oxytocin or an intramuscular injection of syntometrine/ergometrine, if not contraindicated • investigations might include obtaining blood for clotting factors, or the woman might need to return to theatre for further exploration of the uterine cavity.
Wound problemsPerineal problems • the effect of trauma as a physiological process and the normal pattern for wound healing • the nutrients that are necessary to promote healing will assist a midwife to recognize when there is a delay in healing and also enable her to advise a woman on her dietary requirements.
Nutrients and their contribution to healing • Nutrient Contribution • Carbohydrates:Energy for leucocyte, macrophage and fibroblast function • Proteins:Immune response, phagocytosis, angiogenesis, fibroblast proliferation, collagen synthesis, w ound maturation • Fats:Provision of energy, formation of new cells • VitaminsVitamin ACollagen synthesis and cross-linking, tensile strengthVitamin B (complex)Immune response, collagen cross-linking, tensile strengthVitamin CCollagen synthesis tensile strength, neutrophil function, macrophage migration, immune responseVitamin EReduce tissue damage from free radical formation • MineralsCopperCollagen synthesis, leucocyte formationIronCollagen synthesis, oxygen deliveryZincIncreases cell proliferation, epithelialization, collagen strength
Perineal pain is a result of perineal injury, which can be surgically or naturally induced. • Women complain of varying degrees of severity of perineal pain. • the severity of the perineal injury is linked to the severity of perineal pain • Perineal injury that requires suturing predisposes women to an increased risk of severe perineal pain the analgesia no longer being effective, the presence of inflammation in the surrounding tissues or, more seriously, the formation of a haematoma. • Haematoma usually develops deep in the perineal fascia tissues and may not be easily visible if the perineal tissues are already inflamed. • Inadequate perineal repair or a traumatic vaginal birth can increase the risk of a haematoma. • The blood contained within a haematoma can exceed 1000 ml and may significantly affect the overall state of the woman, who can present with signs of acute shock.
Treatment is by evacuation of the haematoma and resuturing of the perineal wound, usually under a general anaesthetic. • Perineal pain that is severe and is not caused by a haematoma might arise as a result of inflammation causing the stitches to feel excessively tight. • Local application of cold packs can bring relief as they reduce the immediate oedema and continue to provide relief over the first few days following the birth • The use of oral analgesia ,use of arnica and lavender
Factors that are associated with poor healing include: • poor diet, obesity, preexisting medical disorders and negative social conditions such as poor housing, increased stress and smoking Where pain in the perineal area occurs at a later stage, or re-occurs, this might be associated with an infection. • The skin edges are likely to have a moist, puffy and dull appearance; there may also be an offensive odour and evidence of pus in the wound. • A swab should be obtained for microorganism culture • strong Antibiotics • discuss with the woman about cleaning the area and making an attempt to reduce constant moisture and heat. • Women might be advised about using cotton underwear, avoiding tights and trousers and frequently changing sanitary pads. • They should also be advised to avoid using perfumed bath additives or talcum powder.
. Most women should be pain-free and be able to resume sexual intercourse within a few weeks after the birth; this will vary in individual women. • Some women may still complain of discomfort, depending on the severity of trauma experienced and the healing process. • Dyspareunia (painful sexual intercourse) can be related to perineal trauma ,and this can in the long-term affect the woman's relationship with her partner. • In the first 3 months post-birth, approximately, 23% of women report dyspareunia
Caesarean section wounds • have prophylactic antibiotics at the time of the surgery • reduce the incidence of wound infection and endometritis. • the wound dressing to be removed after the first 24 hours, as this also aids healing and reduces infection. • care of her wound and adequate drying when taking a bath or shower, or for more obese women where abdominal skin folds are present • a dry dressing over the suture line might be appropriate.
A wound that is hot, tender and inflamed and is accompanied by a pyrexia is highly suggestive of an infection. • a swab should be obtained for microorganism culture. • Haematoma and abscesses can also form underneath the wound and women may identify increased pain around the wound
Circulation • Pulmonary embolism remains a major cause of maternal deaths • alert to identify high-risk women and the possibility of thromboembolism in puerperal women with leg pain and breathlessness • Women who have a previous history of pulmonary embolism, a deep vein thrombosis (DVT), are obese or who have varicose veins have a higher risk of postpartum problems. • Postpartum care of women who have preexisting or pregnancy- medical complications relies on prophylactic precautions • undertaken for women who undergo surgery and have these preexisting factors. • Thromboembolitic D (TED) stockings should be provided during, or as soon as possible after, the birth and prophylactic heparin prescribed until women attain normal mobility.
All women who undergo an epidural anaesthetic, are anaemic, or have a prolonged labour or an operative birth are slightly more at risk of developing complications linked to blood clots. • women who undergo a CS as a result of maternal illness are more likely to spend longer in bed,
thereby reducing their mobility and increasing their risk of morbidity. • Clinical signs that women might report include the following (from the most common to the most serious). • The signs of circulatory problems related to varicose veins are usually localized inflammation or tenderness around the varicose vein, sometimes accompanied by a mild pyrexia. • This is superficial thrombophlebitis, which is usually resolved by applying support to the affected area and administering anti-inflammatory drugs, where these are not in conflict with other medication being taken or with breastfeeding. • Unilateral oedema of an ankle or calf accompanied by stiffness
or pain and a positive Homan's sign might indicate a DVT that has the potential to cause a pulmonary embolism. • Urgent medical referral must be made to confirm the diagnosis and commence anticoagulant or other appropriate therapy. • The most serious outcome is the development of a pulmonary embolism. • The first sign might be the sudden onset of breathlessness, which may not be associated with any obvious clinical sign of a blood clot. • Women with this condition are likely to become seriously ill and could suffer a respiratory collapse with very little prior warning. • Some degree of oedema of the lower legs and ankles and feet it is not accompanied by calf pain (especially unilaterally), pyrexia or a raised blood pressure.
Hypertension • Women who have had previous episodes of hypertension in pregnancy may continue to demonstrate this postpartum for several weeks after the birth • There is still a risk that women who have clinical signs of pregnancy-induced hypertension can develop eclampsia in the hours and days following the birth although this is a relatively rare outcome in the normal population • In addition, some women appear to develop eclampsia postpartum
where there has been no previous history of raised blood pressure or proteinuria • Some degree of monitoring of the blood pressure should be continued for women who were hypertensive antenatally
determine systolic and diastolic levels, with instructions for treatment with antihypertensive medication • women can develop postnatal pre-eclampsia without having antenatal problems associated with this, a headache or epigastric pain or vomiting, the woman may delay or fail to contact a healthcare professional for advice. • Where they do seek advice, the healthcare professional may not be alert to the possibility of the development of postpartum eclampsia
observations of the blood pressure and urine and obtain medical advice. • women with essential hypertension, the management as prescribed
Headache • a common • history of the severity, duration and frequency of the headaches, • the medication being taken to alleviate them and how effective this is. • a recording of the blood pressure should be undertaken to exclude this as a primary factor. • history, if an epidural analgesic was administered • Headaches from a dural tap typically arise once the woman has become mobile after the birth and they are at their most severe when standing, lessening when the woman lies down.
They are often accompanied by neck stiffness, vomiting and visual disturbances. These headaches are very debilitating and are best managed by stopping the leakage of cerebral spinal fluid by the insertion of 10–20 ml of blood into the epidural space • this should resolve the clinical symptoms. Where women have returned home after the birth, they would need to return to the hospital to have this procedure.
Other cause of headache psychological distress • dehydration, sleep loss and a greater than usual stressful environment
Backache • women experience pain or discomfort from backache in pregnancy as a result of separation or diastasis of the abdominal muscles (rectus abdominis diastasis [RAD]). Where backache is causing pain that affects the woman's activities of daily living, referral can be made to local physiotherapy services. Pelvic girdle pain experienced in pregnancy should resolve in the weeks after the baby is born but it may continue for a much longer period
Urinary problems • Urinary problems can have short- and long-term social, psychological and physical health consequences for women • Approximately 19% of women will have urinary problems following birth • Stress incontinence appears to be the most common form of urinary incontinence reported following birth but some women may also suffer from frequency, urgency and urge incontinence • may be susceptible to the risk of urinary infections, which may lead to cystitis and in some severe cases pyelonephritis
a woman has an epidural or spinal anaesthetic, this can have an effect on the neurological sensors that control urine release and flow, which may cause acute retention. • urine retention prevent effective contraction, which leads to increased vaginal blood loss.
women who have sustained pelvic floor damage during birth may suffer from continence problems in the short and long term. • Stress and urge incontinence of urine, utero-vaginal prolapse, cystocele, rectocele and dyspareunia are associated with pelvic floor damage • Very rarely, urinary incontinence might be a result of a urethral fistula following complications from the labor or birth.
A midwife will need to be alert to any urinary problems a • Abdominal tenderness in association with other urinary symptoms, for example a poor output, dysuria or offensive urine and a raised temperature or general flu-like symptoms, might indicate a urinary tract infection (UTI). A mid-stream urine sample will be required to confirm a UTI and the infection can be treated with antibiotics
Women might feel embarrassed about having urinary problems and midwives may need to consider appropriate ways of encouraging women to talk about any problems so that they can inform them about their future management. • further investigations should be made for women who are encountering these problems. Keeping a bladder diary can be a useful aid.
women with ongoing urinary incontinence following birth likely to develop postnatal depression • it is essential that midwives have knowledge and an understanding of the risks and symptoms of urinary problems • These women will need additional social and psychological support
Bowel problems • have short- and long-term social, psychological and physical health consequences for women • about 3–10% of women will suffer from faecal incontinence • Faecal incontinence is associated with primiparity, instrumental birth and severe perineal injury • Constipation and hemorrhoids can be a problem for some women. • 44% of women will suffer from constipation and 20–25% of women will suffer from haemorrhoids following birth. • Symptoms such as flatus incontinence, passive leakage, urge and faecal incontinence can be caused by a neurological or muscular dysfunction or both
ask a woman about her bowel habits. • Factors such as dietary intake, a degree of dehydration during labor and concern about further pain from any perineal trauma can contribute to bowel problems.
A diet that includes soft fiber, increased fluids and the use of non- irritant to the bowel can be prescribed to alleviate constipation • Women need advice that any disruption to their normal bowel pattern should resolve within days of the birth, taking into consideration the recovery required by the presence of perineal trauma. • the effect of a bowel movement on the area that has been sutured as many women may be unnecessarily anxious about the possibility of tearing their perineal stitches. • women have prolonged difficulty with constipation, anal fissures can result • Women who have haemorrhoids should also be given advice on following a diet high in fibre and fluids, preferably water and the use of appropriate laxative to soften the stools as well as topical applications to reduce the oedema and pain.
The role of the midwife is to encourage women to talk about these problems asking women about any bowel problems.
Anemia • Iron-deficiency during pregnancy is common even among well-nourished women and this can be a predisposing risk factor for anaemia in the postnatal period. • severe anaemia (haemoglobin<7 g/dl) it is a serious problem ,may leave many women looking pale and tired for a day • a larger than normal blood loss has occurred,
Investigate the red blood cell volume, haemoglobin and ferritin levels to provide treatment to reduce the effects of the anaemia; these include blood transfusions and iron supplements • Check for preexisting haemoglobinopathies, sickle cell and thalassaemia
haemoglobin level is <9 g/dl and women are symptomatic, a blood transfusion might be appropriate. • Blood transfusions should be considered if a woman is at risk of cardiovascular instability because of their degree of anaemia • Body-store iron deficiency is diagnosed by a low serum ferritin level and this can indicate that the woman has a longstanding problem of iron deficiency. • A cut-off ferritin level varies between 12 and 15 µg/l to confirm iron deficiency • ferritin levels can be raised if infection or inflammation is present, even if iron stores are low
Oral iron and appropriate dietary advice are advocated where the level is <11 g/dl. • ferrous sulphate 200 mg twice daily is recommended; • oral iron should be continued for 3 months • Ascorbic acid (250–500 mg) twice daily may be prescribed to enhance iron absorption • Women should be advised not to have milk (including hot beverages with milk added) at the time of having iron as it can interfere with its absorption.
postpartum woman's haemoglobin values might not have been undertaken where there was no history of anaemia prior to labour and the blood loss at birth was not assessed as excessive. • lethargy, tachycardia and breathlessness as well as a clinical picture of pale mucous membranes, need to investigate hemoglobin level .
Breast problems • experience tightening and enlargement of their breasts towards the 3rd or 4th day as hormonal influences encourage the breasts to produce milk • For women who are breastfeeding the general advice is to feed the baby and avoid excessive handling of the breasts. • Simple analgesics may be required to reduce discomfort. • For women who are not breastfeeding, the advice is to ensure that the breasts are well supported but that this is not too constrictive • taking regular analgesia for 24–48 hours should reduce the discomfort. • Heat and cold applied to the breasts via a shower or a soaking in the bath may temporarily relieve acute discomfort as well as the use of chilled cabbage leaves أوراق ملفوف باردة