Download
1 / 1
10 likes | 157 Views
Pharmacokinetic profile of the base-excision repair inhibitor Methoxyamine-HCl (TRC102; MX) given as an one-hour intravenous infusion

E N D
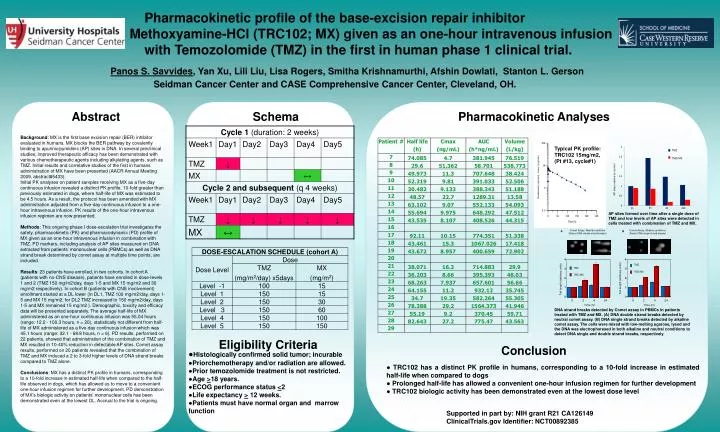
Pharmacokinetic profile of the base-excision repair inhibitor Methoxyamine-HCl (TRC102; MX) given as an one-hour intravenous infusion with Temozolomide (TMZ) in the first in human phase 1 clinical trial. Panos S. Savvides, Yan Xu, Lili Liu, Lisa Rogers, Smitha Krishnamurthi, Afshin Dowlati, Stanton L. GersonSeidman Cancer Center and CASE Comprehensive Cancer Center, Cleveland, OH. Replace with logo Replace with logo Abstract Schema Pharmacokinetic Analyses Background: MX is the first base excision repair (BER) inhibitor evaluated in humans. MX blocks the BER pathway by covalently binding to apurinic/pymidinic (AP) sites in DNA. In several preclinical studies, improved therapeutic efficacy has been demonstrated with various chemotherapeutic agents including alkylating agents, such as TMZ. Initial results and correlative studies of the first in humans administration of MX have been presented (AACR Annual Meeting 2009, abstract#5433).Initial PK analyses on patient samples receiving MX as a five-day continuous infusion revealed a distinct PK profile, 10-fold greater than previously estimated in dogs, where half-life of MX was estimated to be 4.5 hours. As a result, the protocol has been amended with MX administration adjusted from a five-day continuous infusion to a one-hour intravenous infusion. PK results of the one-hour intravenous infusion regimen are now presented. Methods: This ongoing phase I dose-escalation trial investigates the safety, pharmacokinetic (PK) and pharmacodynamic (PD) profile of MX given as an one-hour intravenous infusion in combination with TMZ. PD markers, including analysis of AP sites measured on DNA extracted from patients’ mononuclear cells (PBMCs) as well as DNA strand break determined by comet assay at multiple time points, are included. Results: 23 patients have enrolled, in two cohorts. In cohort A (patients with no-CNS disease), patients have enrolled in dose-levels 1 and 2 (TMZ 150 mg/m2/day, days 1-5 and MX 15 mg/m2 and 30 mg/m2 respectively). In cohort B (patients with CNS involvement) enrollment started at a DL lower (in DL1, TMZ 100 mg/m2/day, days 1-5 and MX 15 mg/m2; for DL2 TMZ increased to 150 mg/m2/day, days 1-5 and MX remained 15 mg/m2 ). Demographic, toxicity and efficacy data will be presented separately. The average half-life of MX administered as an one-hour continuous infusion was 55.04 hours (range: 12.2 - 100.3 hours, n = 20), statistically not different from half-life of MX administered as a five-day continuous infusion which was 45.1 hours (range: 32.1 - 68.8 hours, n = 6). PD results, performed on 22 patients, showed that administration of the combination of TMZ and MX resulted in 10-40% reduction in detectable AP sites. Comet assay results, performed on 20 patients revealed that the combination of TMZ and MX induced a 2 to 3-fold higher levels of DNA strand breaks compared to TMZ alone. Conclusions: MX has a distinct PK profile in humans, corresponding to a 10-fold increase in estimated half-life when compared to the half-life observed in dogs, which has allowed us to move to a convenient one-hour infusion regimen for further development. PD demonstration of MX’s biologic activity on patients’ mononuclear cells has been demonstrated even at the lowest DL. Accrual to the trial is ongoing. Typical PK profile: TRC102 15mg/m2, (Pt #13, cycle#1) AP sites formed over time after a single dose of TMZ and low levels of AP sites were detected in cells treated with combination of TMZ and MX. DNA strand breaks detected by Comet assay in PBMCs in patients treated with TMZ and MX. (A) DNA double strand breaks detected by neutral comet assay. (B) DNA single strand breaks detected by alkaline comet assay. The cells were mixed with low-melting agarose, lysed and the DNA was electrophoresed in both alkaline and neutral conditions to detect DNA single and double strand breaks, respectively. Eligibility Criteria Conclusion ●Histologically confirmed solid tumor; incurable ●Priorchemotherapy and/or radiation are allowed. ●Prior temozolomide treatment is not restricted. ●Age >18 years. ●ECOG performance status <2 ●Life expectancy > 12 weeks. ●Patients must have normal organ and marrow function ● TRC102 has a distinct PK profile in humans, corresponding to a 10-fold increase in estimated half-life when compared to dogs ● Prolonged half-life has allowed a convenient one-hour infusion regimen for further development ● TRC102 biologic activity has been demonstrated even at the lowest dose level Supported in part by: NIH grant R21 CA126149 ClinicalTrials.gov Identifier: NCT00892385



















