Download
1 / 24
290 likes | 1.04k Views
Systolic Ejection Murmurs Chapter 14. Are G. Talking, MD, FACC Instructor Patricia L. Thomas, MBA, RCIS. Outflow Tracts Inflow Tracts Inter-Ventricular Flow Ejection Murmur Classification of Ejection Aortic Stenosis Bicuspid Aortic Valve. Tetralogy of Fallot

E N D
Systolic Ejection MurmursChapter 14 Are G. Talking, MD, FACC Instructor Patricia L. Thomas, MBA, RCIS
Outflow Tracts Inflow Tracts Inter-Ventricular Flow Ejection Murmur Classification of Ejection Aortic Stenosis Bicuspid Aortic Valve Tetralogy of Fallot Dilatation of the Proximal Pulmonary Pulmonary Arterial Narrowing Coarctation of the Aorta Musical Murmurs Outline
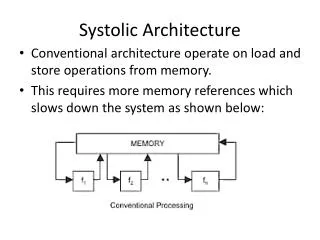
Introduction • Levine stated, “Systolic noise with a duration longer than a heart sound.” • Result of turbulent blood flow across outflow tracts, ejection murmurs,inflow tract, and from ventricle to ventricle
Left outflow tract Left ventricle Aortic valve Aortic root Ascending Aorta Right outflow tract Right ventricle Pulmonary Valve Main Pulmonary Artery Outflow Tracts/ Ejection Pathways
Causes of Abnormalities of Flow • Forward flow across normal outflow tracts • Forward flow across stenosed aortic or pulmonic outflow tracts • High flow across normal right or left ventricular outflow tracts • High flow across a regurgitant aortic or pulmonic valve without significant stenosis • Forward flow into a dilated great vessel
Inflow Tracts • The inflow tracts of the heart are the chambers that are open to tack other during diastolic filling. • Mitral valve is part of the left inflow tract • Tricuspid valve is part of the right inflow tract • Abnormalities are insufficiency/regurgitant related: rheumatic valvular disease, mitral valve prolapse, or papillary muscle dysfunction
Inter-Ventricular Flow • Small VSD results in turbulent blood flow from ventricular to ventricle
Ejection Murmur • Mixed frequencies and is moderate-to-marked crescendo-decrescendo • Caused by forward flow across the left or right outflow • Aortic stenosis & pulmonic stenosis
Classification of Ejection Murmurs • Early Systolic Ejection Murmur • Commonly heard in a small VSD without pulmonary hypertension, large VSD with pulmonary hypertension, septal perforation resulting from MI, acute severe mitral regurgitation • Mid-systolic Ejection Murmur • Long and is loudest in mid-systolic with the sound of S2 clearly audible & implies significant aortic or pulmonic outflow tract obstruction, TOF, dilatation of he proximal pulmonary artery or ASD
Aortic Stenosis • Murmur is harsh, rough, & grunting • Degrees of Obstruction • Mild- softer, shorter & earlier-peaking systolic murmur • Severe-louder, longer, & late-peaking murmur • Causes • Result of congenital aortic valve disease, rheumatic fever (aortic & mitral valve involved), or degenerative calcification in elderly patients • Listen with the diaphragm of the stethoscope for maximal intensity at the second right intercostal space; listen at the apex & over the precordium, both clavicles, both carotids, & suprasternal notch
Pulmonic Valve Stenosis • Harsh systolic murmur,wide splitting of S2 • Loudest in the 2nd & 3rd interspaces along the left sternal border (pulmonic area) • Palpable Thrill felt directed toward the left neck or clavicle • Murmur peaks in mid-systole with maximal ejection & produces a diamond shape on the phono. • Heard during expiration • Ejection sound heard over the pulmonary area • Sound caused by doming & abrupt arrest in motion of the stenotic PV
Tetralogy of Fallot • Described by Fallot in 1888 • VSD, Pulmonic Stenosis, Dextroposition of the aorta & RV hypertrophy • PS results of a fibromuscular ring below the PV in the RV out flow tract-infundibular • More severe the obstruction, the more blood is shunted RT to LT the VSD • Systolic thrill pulmonic with grade IV murmur
Coarctation of the Aorta • Grade II or III murmur • Heard posteriorly & over base of the heart • Hypertension in the arms, but not in the legs • Decreased or absent femoral arterial pulsation
Musical Murmurs • Caused by vibrating structure enve in the the absence of flow turbulence • Musical systolic murmurs • Cooing of a dove • Buzzing of a saw • Spinning of a top • Whistling • Systolic whoop • Precordial honk • Mitral valve prolapse can assume such a noise
THE END OF CHAPTER 14 Tilkian, Ara MD Understanding Heart Sounds and Murmurs, Fourth Edition, W.B. Sunders Company. 2002, pp. 154-178