Download
1 / 29
300 likes | 423 Views
Palliative care and terminal illness: Grief, loss and communication. Linda Hadeed, PhD Palliative Care Conference October 2012. PALLIATIVE CARE. Specialized medical care for people with serious illnesses Focus – to provide patients relief from pain, and stress of a serious illness

E N D
Palliative care and terminal illness:Grief, loss and communication Linda Hadeed, PhD Palliative Care Conference October 2012
PALLIATIVE CARE • Specialized medical care for people with serious illnesses • Focus – to provide patients relief from pain, and stress of a serious illness • Goal - to improve quality of life for both the patient and the family • Team of doctors, nurses, and other specialists work together with patient's other doctors to provide an extra layer of support
PALLIATIVE CARE • Appropriate at any age or stage in a serious illness • Sometimes provided along with curative treatment • Time for close communication • Help navigate the healthcare system • Guide with difficult and complex treatment choices
PALLIATIVE CARE • Emotional and spiritual support for patient and family – care for mind, body and spirit • Generally the team works closely together to provide what is needed • Different from care to cure illness (curative treatment)
PALLIATIVE CARE • Serious illness makes patients and families feel lonely, angry, scared, or sad • May feel that care [treatment] doing more harm than good • Palliative care providers generally interested in what is bothering the patient, what is important to the patient and family and work to help them cope
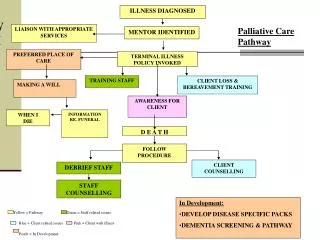
Palliative Care vs.Hospice Care • Hospice care provides:- • medical services • emotional support • spiritual resources for people who are in the late stages of an incurable illness • Helps family members manage the practical details and emotional challenges of caring for a dying loved one
Hospice Care • Hospice services provided by team of caregivers that may include health professionals, volunteers, and spiritual advisors • Services generally include:- • Basic medical care focuses on pain and symptom control • Medical supplies and equipment, as needed.
Hospice Care • Counseling and social support • Services are available, as needed, for both the person in hospice care and for anyone in his or her family. • Guidance with the difficult, but normal, issues of life completion and closure
Hospice Care • A break (respite care) for caregivers, family, and others who regularly care for the person • Volunteer support, such as meal preparation or errand running • Generally, hospice care is free of charge • Primary aim is to enhance the quality of life and dignify the terminal stages through special care
Terminal Illness & Trauma • Trauma is no longer defined as experience outside the norm of human experiences • More recently, trauma is as anything that traumatizes the individual (defined by the individual) • Can be physical, emotional or psychological
Terminal Illness & Trauma • Emotional and psychological trauma shatters the person’s sense of safety and security • Results in person feeling helpless and vulnerable in a dangerous world.
Causes of emotional or psychological trauma • It happened unexpectedly • You were unprepared for it • You felt powerless to prevent it • It happened repeatedly • Someone was intentionally cruel • It happened in childhood • SERIOUS ILLNESS CAN BE TRAUMATIC
Emotional and psychological symptoms of trauma • Shock, denial, or disbelief • Anger, irritability, mood swings • Guilt, shame, self-blame • Feeling sad or hopeless • Confusion, difficulty concentrating • Anxiety and fear • Withdrawing from others • Feeling disconnected or numb
Physical symptoms of trauma • Insomnia or nightmares Being startled easily Racing heartbeat Aches and pains Fatigue Difficulty concentrating Edginess and agitation Muscle tension
Grief and loss • Length and intensity of grief determined by:- severity of the traumatic event • Earlier traumas • Coping skills of the individual(s) • Social support (availability, accessibility, actual use and satisfaction of the support) • GRIEF & LOSS & TERMINAL ILLNESS
Grief and loss • For professionals: • their own earlier traumas, especially around issues of terminal illness • Whether this was processed or not, etc., will determine how they cope and the quality of service they can provide to the patient and family
Stages of grief and loss(Elizabeth Kubler-Ross, 1969) • The Five Stages of Grief and Loss (not just for death and dying) • -Denial • -Anger • -Bargaining • -Sadness/Depression • -Acceptance/Resolution
Communication in Palliative Care(Robert Buckman) • Three areas of communication:- • (1) Basic listening skills • (2) The specific communication tasks • - breaking bad news & therapeutic dialogue • (3) Communicating with the family and with other professionals
Communication in Palliative Care(Robert Buckman) • Sources of difficulty in communicating with the dying patient • (1) those related to society • (2) those related to the patient • (3) those related to the health care professional • (medical school training)
Communication in Palliative Care(Robert Buckman) • The social denial of death (tabboo topic) • “No you aren’t,” …“Don’t talk that way” (Christine Middlebrook in memoir, “Seeing the crab” • We want to protect ourselves from the reality of death…we say the wrong things • Lack of experience of death in the family (rise in modern health care facilities; good but disruption of support for the patient and family)
Communication in Palliative Care(Robert Buckman) • The changing role of religion (your soul will be with your maker may no longer bring comfort) • Patient’s fear of dying (not a single emotion; elicit from the patient what aspects of terminal illness are uppermost in his/her mind)
Communication in Palliative Care(Robert Buckman) • Factors originating in the health care profession • (don’t get the patient upset) • Fear of saying “I don’t know” • Fear of expressing emotion • Own fears of illness and death
6-Step Protocol for Breaking Bad News(Robert Buckman) • Getting the physical context right • Finding out how much the patient knows (“what have you made of the illness so far?” • Finding out how much the patient wants to know • Sharing information • Responding to the patient’s feelings • Planning and following through
Helping Patients and Families • Attentive listening (allow person or family to tell story, vent, lament, etc., and • Tolerate short silences • Validate – if tears or angry outbursts, don’t attempt to stop either (allow the tears, use words Might say, “ let the tears come, you might need to cry, this is a huge loss”
Helping Patients and Family • Repetition and reiteration • (use the patients’ words in your response and repeat what the patient has said to show you understand what the patient has said) • Empathic response (you seem to be feeling…) • Communication is important from the first time you meet the patient to the last time
Helping Patients and Family • To help family grieve, might ask questions like:- • What do you like best about this person? • And what else… and what else … (help person talk things through) What would you miss?
Helping Patients and family • Might also ask: • What is (or would be) lost? • What is (or would be) left? • What is (or might be ) possible?
Helping Patient and Family • You don’t need to take responsibility for fixing anything for anybody…not their feelings, not what they ought to do, etc., (don’t put unnecessary stress on yourself) • TAKE CUE FROM THE PERSON AND RESPOND TO WHAT IS BEING SAID (not what you think the person needs to hear or should know (not about your agenda)
Self-care for professionals • Do not minimize the toll on yourself • Talk over feelings, thoughts with colleagues, friends, etc., whether you think it is bothering you or not • Nurture yourself (simple things like warm shower with a nice soap) • Do a fun thing for yourself weekly, eat properly, get enough sleep, exercise, etc.,