Download
1 / 15
150 likes | 170 Views
Huntington’s Disease. For any condition. Pathophysiology Epidemiology Symptoms Signs Diagnosis Prognosis Complications Treatment Prevention. Pathophysiology. Huntington's Disease (HD) is an inherited neurological condition. HD is caused by a faulty gene on chromosome 4 (IT-15).

E N D
For any condition... • Pathophysiology • Epidemiology • Symptoms • Signs • Diagnosis • Prognosis • Complications • Treatment • Prevention
Pathophysiology • Huntington's Disease (HD) is an inherited neurological condition. • HD is caused by a faulty gene on chromosome 4 (IT-15). • People with HD have a "molecular stutter" of three nucleotides (CAG) located in exon 1 • This results in an uninterrupted polyglutamine stretch within the N-terminus of the huntingtin molecule. • The "normal" number of CAG repeats is between 9 and 30. • Between 30 and 39 repeats is a grey area, where people may or may not go on to develop HD. • Over 39 is considered defective, and some patients may have as many as 100 CAG repeats.
The CAG repeat length is estimated to account for approximately 70% of the variance in age of onset. • Extremely large CAG repeats of 80 or greater are often associated with a disease onset during childhood or adolescence (juvenile HD). • There is a tendency for greater repeat expansion when the father, rather than the mother, transmits the disease causing mutations. • These mutations in the gene result in the huntingtin protein being longer in length. This longer protein then accumulates abnormally in the brain cells and eventually leads to brain cell death. • HD has previously been thought to have 100% penetrance, however it is now known that the penetrance is dependant on CAG repeat length.
2. Normal male karyotype 3. Normal female karyotype Normal Male Karyotype Huntington’s Disease Karyotype Normal Female Karyotype
Epidemeology • The altered gene is passed from parent to child without regard for sex. • If a person does not inherit the altered gene for HD then his or her children are not at risk of developing HD. • HD affects approximately 1 in 20,000 people of European descent, and usually manifests itself between the ages of 30 and 50 years. • Being an autosomal dominant disorder, children of a person with a defective HD gene have a 50:50 chance of inheriting the gene from their affected parent. • Juvenile Huntington’s occurs in approximately 16% of all cases of Huntington's. • 80% of cases with onset before 20 years of age (juvenile HD) are due to paternal transmission. • Huntington's disease is about 10 times more prevalent in Western European populations compared to African and Asian populations. • Huntington's occurs about twice as often in Tasmania compared to the rest of Australia due to an individual with Huntington's settling in Tasmania many years ago and passing the mutation on.
Signs & Symptoms • The most common symptom of the condition is chorea; that is dance-like or jerky movement of the arms and legs. These movements begin as twitches and gradually increase over a period of years to larger movements. • Physical SymptomsIn the early stages of HD a person is likely to experience some mild twitching of the fingers and toes, and perhaps the face or limbs. He or she may feel a little less co-ordinated, fumbling or knocking things over. As the disease progresses, walking may become more challenging and, as coordination decreases. • Cognitive Symptoms“Cognitive" - referring to tasks of the brain concerned with knowing, thinking, planning, judging and remembering. • Short term memory may be reducedOver time concentration for activities such as reading and demanding conversation may be affected. • HD does not affect a person's orientation. • Personality or Emotional SymptomsChanges to personality will begin subtly. In the early stages of HD, a person may be more irritable or moody than previously. Depression is common to about a third of all people affected by the condition. Some persons affected by HD laugh or smile at inappropriate times or may feel like crying for no apparent reason.
Diagnosis • Pre-symptomatic genetic testing is for individuals at risk for HD who do not have symptoms. Pre-symptomatic genetic testing involves genetic counselling. • The requirements for the diagnosis of HD include: -Medical history -Family history -Neurological examination -Brain imaging test (MRI, CT, PET) -Laboratory tests -Genetic test (if necessary) • During such testing, blood samples are taken from patients and DNA is directly analysed for HD mutations. The DNA is studied through a series of tests known as Polymerase chain reactions or PCR testing. • During this testing, the number of CAG repeats within the IT15 gene region is estimated. Additional blood samples may be obtained from close or first-degree relatives with HD to help confirm the results. • If between 35-40 CAG’s may or may not develop the disease . • The area most noticeably damaged is the corpus striatum. • In some patients, the disease leads to a loss of 25% or more of total brain weight.
Prognosis • Once symptoms begin, there is progressive cognitive, motor and psychiatric impairment; with death occurring an average of 18 years after onset of symptoms. • Death for most people with Huntington's disease is usually a result of infection, pneumonia, heart failure or choking. • The most common cause of death is pneumonia due to the individual not being able to clear their lungs properly and having problems with swallowing, which results in food and liquid entering their lungs. • The second most common cause of death is heart failure. • The suicide rate among HD patients is 5-10 times higher than in the general population. • Eventually the person is unable to care for themselves and requires total nursing care.
Complications • With regard to screening: between 35-40 CAG’s – grey area • Though the signs and symptoms vary from person to person, vital functions, such as swallowing, eating, speaking and walking, usually degenerate over time. • Depression is common in Huntington's disease, and some people are at risk of suicide. However, death generally occurs as a result of complications of the disease, such as a fall or an infection like pneumonia. • Weight loss and eating difficulties due to swallowing difficulties and lack of other muscle coordination make management of nutrition important. • Thickening agents can be added to liquids to make the fluids easier and safer to swallow and reduce the chance of fluids entering the lungs. If eating becomes too dangerous or uncomfortable, a feeding tube can be used.
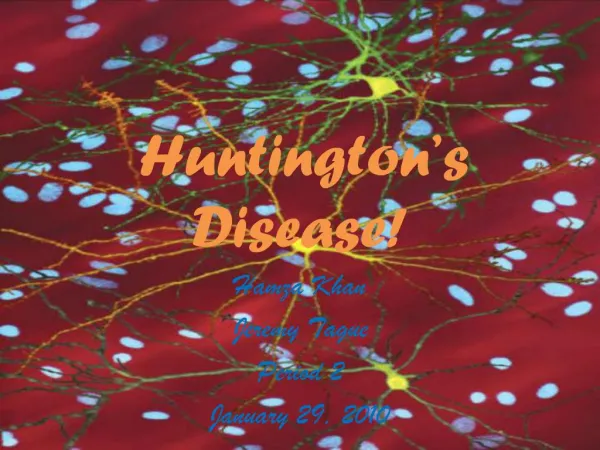
Treatment • Two Eurepoean scientists made the breakthrough discovery that dopamine pathways between neurons are destroyed in Parkinson’s disease patients. Since the symptoms of Parkinson’s disease are nearly the opposite of those with HD, the scientists hypothesise that decreasing HD patient’s dopamine levels may be a key step in treating the disease (Late 1950s) • Tetrabenazine (Xenazine) was developed specifically to reduce the severity of the jerky/involuntary movements occurring in Huntington's disease. • Other drugs are also used to help reduce involuntary movements – these include neuroleptics and benzodiazepines. The rigidity experienced by some patients can be treated with antiparkinsonian drugs. • There are drugs which can be used to treat depression. • Physical Therapy is very important as well as speech therapy to help the patient lead a more normal life. • There is no effective treatment for HD, although some symptomatic relief may be obtained.
Prevention • People at risk of passing the genetic defect that causes Huntington's disease to your children, may wish to consider adoption or certain forms of assisted reproduction. One possibility is in vitro fertilization with pre-implantation screening. In this procedure, embryos are screened for the Huntington's disease gene mutation, and those that don't have the mutation are then implanted in the woman's uterus. • A number of compounds that have shown promise in animal studies and in pilot clinical trials are currently under investigation for the treatment of Huntington's disease. • Gene therapies to reduce the amount of mutant Huntington protein in the brain have shown great promise in the laboratory setting
Caring for people with HD • People with HD can improve their quality of life by attempting to remain active physically, mentally and socially. Walking, reading and maintaining friendships are some examples. • The person with HD should attempt to live as fulfilling a life as possible. • At this point there is no cure for HD, but some symptomatic treatments and support services are available to individuals and families affected by HD.
Presymptomatic Testing • Presymptomatic TestingThe gene responsible for HD was identified in 1993 making it possible for those people who are at risk to the condition to take a test to determine whether or not they have inherited the gene. Candidates for testing must be a minimum of eighteen years of age, and must want to know their gene status in order to be accepted for testing. Extensive support, information and counselling are available.