Download
1 / 19
190 likes | 208 Views
This comprehensive overview delves into the characteristics, risk factors, clinical features, and prognostic factors of Acute Myeloid Leukemia in 2015. It explores the evaluation process, cytogenetic risk groups, survival rates, and current therapy options for both younger and older adults. Moreover, investigational approaches in AML therapy and selected agents in clinical trials are discussed in detail. Stay informed on the latest advancements in AML research and treatment modalities.

E N D
Olga Frankfurt, MD Robert H. Lurie Comprehensive Cancer Center Northwestern University Chicago, IL Acute Myeloid Leukemia - 2015
Acute Myeloid Leukemia (AML) • AML is a group of blood cancers in which the bone marrow makes abnormal immature blood cells • These cells also prevent the normal blood cells from maturation
Acute Myeloid Leukemia (AML) • New patients/deaths in 2014: 18,860/10,460 • Median age: 66 -72 years • Heterogeneity in genetics, clinical features and outcome • Outcome improved among age <60 with intensive post-remission strategies and transplantation • Prognostic factors exist; many new, molecular • Role of transplantation continues to be refined • Myriad of new agents available
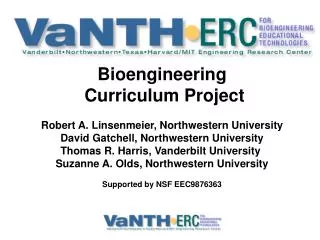
AML Age-Specific Incidence Rates 24 Incidence/100,000 22 20 18 16 14 12 10 8 6 4 2 0 0-4 5-9 85+ 60-64 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 65-69 70-74 75-79 80-84 Age (y) NCI-SEER Program
Risk Factors for Developing AML • Previous exposure to radiation • Environmental factors : tobacco, benzene • Genetic factors • Down’s syndrome • Fanconi’s anemia, Bloom syndrome • Ataxia telangectasia
Risk Factors for Developing AML • Previous chemotherapy • Alkylating agents • del 5 and del 7 • 5 - 10 years latency • Epipodophyllotoxins (etoposide, anthracyclines) • Monocytic differentiation • 11q23 • 1-3 years after exposure • Evolving from the prior antecedent hematologic disorder
Clinical Features of AML • Constitutional symptoms • Infections • Abnormal blood counts • Complications related to the high WBC • Coagulation abnormalities • Metabolic abnormalities • Extramedullary tissue
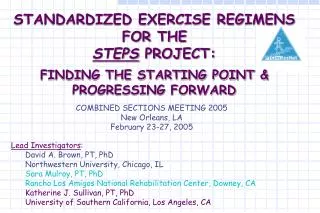
Morphology peripheral blood smear bone marrow core biopsy
Evaluation of Patient with AML • History and Physical Examination • CBC with differential and platelet, peripheral smear, CMP, uric acid, DIC panel, pregnancy test • Bone marrow aspirate and biopsy/ Flow cytometry • Cytogenetics • Molecular studies: • FLT3, NPM1, c-kit, CEBPα, IDH1, IDH2, k-RAS, n- RAS • Next generation sequencing • HLA typing and eligibility for stem cell transplant • Serologies: hepatitis, HIV, CMV • Study specific correlative laboratory studies
Cytogenetic Risk Groups Favorable inv(16); t(15;17) with any abn; t(8;21) lacking del(9q) or complex karyotype Intermediate Normal or +8 or +21 or others Unfavorable -5/del(5q), -7/del(7q), inv(3q), abn of 11q, 20q, 21q, 17p, del(9q), t(6;9), t(9;22), complex karyotypes with 3 abn Slovak ML, et al. Blood. 2000;96(13):4015-4083.
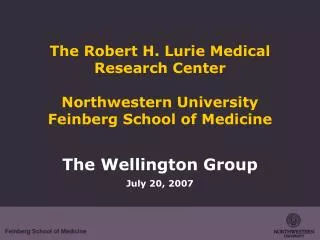
Overall Survival by Cytogenetic Group Estimate At Risk Deaths at 5 Years 100 Favorable 121 53 55% Intermediate 278 168 38% Unfavorable 184 162 11% 80 60 Favorable Cumulative Percentage 40 Intermediate 20 Unfavorable Heterogeneity of 3 Groups: P < 0.0001 0 0 2 4 6 8 Years After Entering Study Slovak ML, et al. Blood. 2000;96(13):4015-4083.
Therapy for AML- Principles • Without therapy AML is fatal – days-months • The therapy for AML: Induction and Consolidation • Chemotherapy may cure selected patients and prolong survival in responding patients • Chemotherapy is toxic and can cause substantial morbidity and mortality
Current AMLTherapy-2015 Younger Adults • Induction: dauno 60-90 mg/m2/d x 3d + ara-C 100/200 mg/m2/d x 7d CI. • Consolidation: high- or intermediate-dose ara-C (1-4 cycles) • Allogeneic HCT for intermediate- and high-risk • Consider in CBF with c-KIT, FLT3 • Not done in FLT3-/NPM1+ , CEBP+(double mutation) Paschka J ClinOncol, 2006; Schlenk N Engl J Med, 2008; Green J ClinOncol, 2010; Dohner Blood, 2010
Current AMLTherapy-2015 Older Adults • Decision: chemotherapy vs. hypomethylating agent • Intensive Chemotherapy • Induction: dauno 60-90 mg/m2/d x 3d + ara-C 100 mg/m2/d x 7d • Consolidation: intermediate-dose ara-C (1-4 cycles); no clear role in older adults • Low dose Chemotherapy • Hypomethylating agents: • Dacogen:5 days course or 10 days course • Vidaza : 7 days course • Reduced intensity HSCT
Investigational Approaches AMLTherapy-2015 • Autologous HSCT is not a standard of care; being studied • Maintenance is not a standard of care; being studied • Maintenance after allo HSCT is not a standard of care for AML; being studied; many use hypomethylating agents • Adding stem cells to expedite count recovery after the chemotherapy ; being studied • Adding agents that stimulate platelet recovery after chemotherapy is being studied • Altering the immune system to fight leukemia ( CAR-T cells)
Selected Agents in Clinical Trials • Chemotherapy - Clofarabine, CPX-351, Vosaroxin, Elacytarabine • Hypomethylating agents – Decitabine, Azacitidine • FLT3 inhibitors – Sorafenib, Quizartinib, Crenolanib, ASP2215 • MLL inhibitors – EPZ-5676 • IDH1 and IDH2 inhibitors, pan IDH inhibitor • Glutaminase inhibitor CB-839 • Exportin 1 inhibitor - Selinexor • Polo-like kinase inhibitor - Volasertib • C-kit inhibitors – Dasatinib • mTOR inhibitors – Temsirolimus • Histone deacetylase inhibitors – Vorinostat, Panobinostat • Antibody conjugates • Cycline-dependent kinase inhibitor – Flavoperidol • Hedgehog inhibitors • MEK1/2 inhibitors – Trametinib • Aminopeptidase inhibitors – Tosedostat
312 695-6180 Academic Office • 312 695-0990 Cancer Center Olga Frankfurt, MD Co-director - Leukemia Program Director - Chronic Leukemia/MDS Associate Director for Umbilical Cord Blood Transplantation Robert H. Lurie Comprehensive Cancer Center, Northwestern Medicine