Download
1 / 41
410 likes | 597 Views
Examination of the Knee. Thursday SM Conference August 30, 2007. Exam Settings. Sideline Exam (on the field triage) Training room (post game eval) Office/clinic Exam (delayed + detailed). Sideline Exam Purpose: determine disposition. Transfer (severe injury)

E N D
Examination of the Knee Thursday SM Conference August 30, 2007
Exam Settings • Sideline Exam (on the field triage) • Training room (post game eval) • Office/clinic Exam (delayed + detailed)
Sideline ExamPurpose: determine disposition • Transfer (severe injury) • Hold out (mild – moderate) • Observe + re-examine • Provide first aide • Return to action (mild ?– no injury?)
Sideline Exam Routine • Determine mechanism • Point of maximum tenderness • Maneuver producing most pain • Determine severity of damage
Case Presentation 22 year old collegiate wrestler Contact injury to left knee Medial-sided knee pain
Mechanism ? • Foot planted • Outside force • Pain + “pop”
Sideline Exam • Pain “on inside”
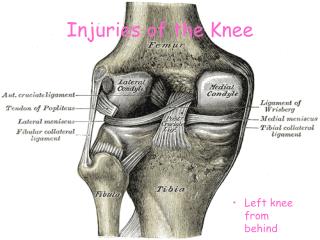
Medial Pain(Differential Diagnoses) • Medial Collateral Ligament sprain • Hamstring strain • Gastroc strain • Medial Meniscus tear
Maximum Tenderness? • Pain “on inside” • Tender over MCL
Most Painful maneuver? • Straight Valgus? • Straight • 30 degrees • External rotation?
Sprain Severity? • Classify by laxity • Best exam technique • One-handed • Two handed
Check both sides! • Laxity normal ??? • “Plastic man” • Post exercise
Exam Settings • Sideline Exam (on the field triage) • Training room (post game eval) • Office/clinic Exam
Two handed technique • Trap ankle on Iliac crest • Both hands on joint line • Palpate both joint lines Stress X-ray
Hughston Laxity Classification • Grade I – 1-4 mm laxity • Grade II – 5-9 mm laxity • Grade III – >10 mm laxity (soft endpoint) • Hughston JC, Andrews JR, Cross MJ, Moschi A: Classification of knee ligament instabilities. Part I. The medial compartment and cruciate ligaments. • J Bone Joint Surg Am 58:159-172, 197
Two handed technique • Trap ankle on Iliac crest • Both hands on joint line • Palpate both joint lines Stress X-ray
Collegiate footballSeverity vs. Return • Grade I – 10.6 days • Grade II – 19.5 days Derscheid, G.L. and J.G. Garrick. MCL injuries in football: Non-operative management of grade I and grade II sprains. Am J Sports Med, 1981. 9(6): p. 365-8.
Sideline estimate(Crowley-Albright 30 consecutive FB cases) 1 mm = 1 week 2 mm = 2 weeks 3 mm = 3 weeks 6 mm = 6 weeks millimeters = weeks
Time Loss From Sport • Severity of injury • Compliance??
Exam Settings • Sideline Exam (on the field triage) • Training room (post game eval) • Office/clinic Exam
Office Exam • What is important about the MCL exam? • Knee stability in full extension
KneeHemarthrosisDifferential Diagnosis • ACL 70% • Meniscus 50% • Fracture 20% • Patellar dislocation • PCL
Value of MRI? • When should an MRI be done? • When knowledge of location of injury might influence treatment • When additional injury is suspected • Instability at full extension should increase suspicion of cruciate injury • Mazzocca, A.D., et al., Valgus medial collateral ligament rupture causes concomitant loading and damage of the anterior cruciate ligament. • J Knee Surg, 2003. 16(3): p. 148-51.
Location MCL Tissue damage • Proximal ruptures heal more quickly than distal but have more stiffness • Complete ruptures can displace into the joint • Damage over entire ligament associated with persistent laxity after non-operative treatment • Nakamura, N., S. Horibe, et al. (2003). "Acute grade III MCL injury of the knee associated with ACL tear. usefulness of MRI in determining treatment regimen." • Am J Sports Med 31(2): 261-7.
Grade III – Gross instabilityLaxity at full ext (no endpoint) Indicates completerupture of MCL • Evaluate posteromedial capsule • Evaluate for cruciate injury • ACL • PCL • Evaluate for Patellar Dislocation
Pivot shift techniques • Re-entry tests • MacIntosh • Hughston Jerk • Exit tests • Losee (5 tests) • Slocum • Low profile Slocum's pivot test
The “Pivot-Shift”“Low Profile” Technique • “exit” type pivot (in-to-out of place) • No valgus • Limit arc to last 20 degrees
Losee Tests See video
Reverse pivot • Ask patient “In or out?”
Meniscus tears • Joint line tenderness • Most sensitive but least specific (Fu) • Squat and duck walk test • McMurray' s test • Modified McMurray' s test • Most sensitive but least sensitive • Appley’s test • Modified Appley’s test • Full Extension?? • Pain anterior joint line
Displaced Meniscus?(bucket-handle tear) • Lacks full extension • No screw home • Pain anterior joint line • Rotation affects degree of pain • Lacks full flexion • Rotation affects degree of pain • Rotation OK in mid range flexion
Anterior knee pain • Osgood Schlatter' s • Jumper’s knee • P-F Chondromalacia • Synovitis (Plica?) • P-F instability