Download
1 / 1
10 likes | 203 Views
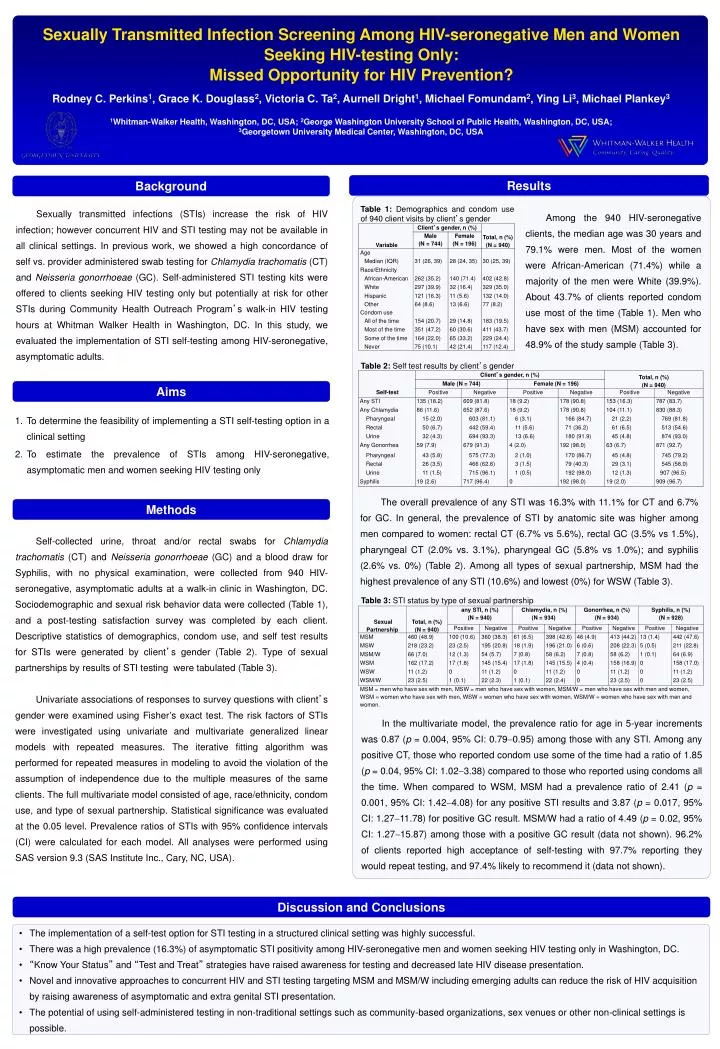
Sexually Transmitted Infection Screening Among HIV-seronegative Men and Women Seeking HIV-testing Only: Missed Opportunity for HIV Prevention?. Rodney C. Perkins 1 , Grace K. Douglass 2 , Victoria C. Ta 2 , Aurnell Dright 1 , Michael Fomundam 2 , Ying Li 3 , Michael Plankey 3.

E N D
Sexually Transmitted Infection Screening Among HIV-seronegative Men and Women Seeking HIV-testing Only: Missed Opportunity for HIV Prevention? Rodney C. Perkins1, Grace K. Douglass2, Victoria C. Ta2, Aurnell Dright1, Michael Fomundam2, Ying Li3, Michael Plankey3 1Whitman-Walker Health, Washington, DC, USA; 2George Washington University School of Public Health, Washington, DC, USA; 3Georgetown University Medical Center, Washington, DC, USA Results Background Table 1: Demographics and condom use of 940 client visits by client’s gender Sexually transmitted infections (STIs) increase the risk of HIV infection; however concurrent HIV and STI testing may not be available in all clinical settings. In previous work, we showed a high concordance of self vs. provider administered swab testing for Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (GC). Self-administered STI testing kits were offered to clients seeking HIV testing only but potentially at risk for other STIs during Community Health Outreach Program’s walk-in HIV testing hours at Whitman Walker Health in Washington, DC. In this study, we evaluated the implementation of STI self-testing among HIV-seronegative, asymptomatic adults. Among the 940 HIV-seronegative clients, the median age was 30 years and 79.1% were men. Most of the women were African-American (71.4%) while a majority of the men were White (39.9%). About 43.7% of clients reported condom use most of the time (Table 1). Men who have sex with men (MSM) accounted for 48.9% of the study sample (Table 3). Table 2: Self test results by client’s gender Aims To determine the feasibility of implementing a STI self-testing option in a clinical setting To estimate the prevalence of STIs among HIV-seronegative, asymptomatic men and women seeking HIV testing only The overall prevalence of any STI was 16.3% with 11.1% for CT and 6.7% for GC. In general, the prevalence of STI by anatomic site was higher among men compared to women: rectal CT (6.7% vs 5.6%), rectal GC (3.5% vs 1.5%), pharyngeal CT (2.0% vs. 3.1%), pharyngeal GC (5.8% vs 1.0%); and syphilis (2.6% vs. 0%) (Table 2). Among all types of sexual partnership, MSM had the highest prevalence of any STI (10.6%) and lowest (0%) for WSW (Table 3). Methods Self-collected urine, throat and/or rectal swabs for Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (GC) and a blood draw for Syphilis, with no physical examination, were collected from 940 HIV-seronegative, asymptomatic adults at a walk-in clinic in Washington, DC. Sociodemographic and sexual risk behavior data were collected (Table 1), and a post-testing satisfaction survey was completed by each client. Descriptive statistics of demographics, condom use, and self test results for STIs were generated by client’s gender (Table 2). Type of sexual partnerships by results of STI testing were tabulated (Table 3). Univariate associations of responses to survey questions with client’s gender were examined using Fisher’s exact test. The risk factors of STIs were investigated using univariate and multivariate generalized linear models with repeated measures. The iterative fitting algorithm was performed for repeated measures in modeling to avoid the violation of the assumption of independence due to the multiple measures of the same clients. The full multivariate model consisted of age, race/ethnicity, condom use, and type of sexual partnership. Statistical significance was evaluated at the 0.05 level. Prevalence ratios of STIs with 95% confidence intervals (CI) were calculated for each model. All analyses were performed using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA). Table 3: STI status by type of sexual partnership In the multivariate model, the prevalence ratio for age in 5-year increments was 0.87 (p = 0.004, 95% CI: 0.790.95) among those with any STI. Among any positive CT, those who reported condom use some of the time had a ratio of 1.85 (p = 0.04, 95% CI: 1.023.38) compared to those who reported using condoms all the time. When compared to WSM, MSM had a prevalence ratio of 2.41 (p = 0.001, 95% CI: 1.424.08) for any positive STI results and 3.87 (p = 0.017, 95% CI: 1.2711.78) for positive GC result. MSM/W had a ratio of 4.49 (p = 0.02, 95% CI: 1.2715.87) among those with a positive GC result (data not shown). 96.2% of clients reported high acceptance of self-testing with 97.7% reporting they would repeat testing, and 97.4% likely to recommend it (data not shown). Discussion and Conclusions • The implementation of a self-test option for STI testing in a structured clinical setting was highly successful. • There was a high prevalence (16.3%) of asymptomatic STI positivity among HIV-seronegative men and women seeking HIV testing only in Washington, DC. • “Know Your Status” and “Test and Treat” strategies have raised awareness for testing and decreased late HIV disease presentation. • Novel and innovative approaches to concurrent HIV and STI testing targeting MSM and MSM/W including emerging adults can reduce the risk of HIV acquisition by raising awareness of asymptomatic and extra genital STI presentation. • The potential of using self-administered testing in non-traditional settings such as community-based organizations, sex venues or other non-clinical settings is possible.