Download
1 / 1
10 likes | 155 Views
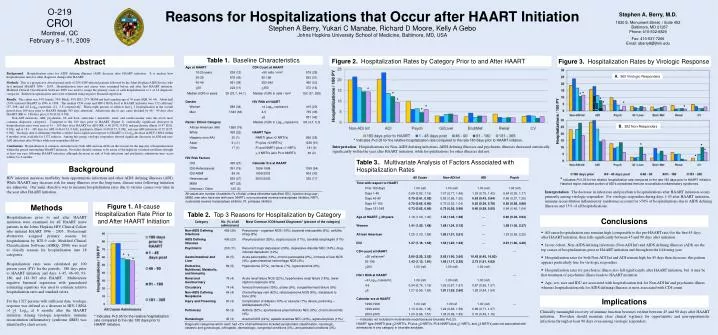
Figure 2. Hospitalization Rates by Category Prior to and After HAART. Abstract. Background : Hospitalization rates for AIDS defining illnesses (ADI) decrease after HAART initiation. It is unclear how hospitalization rates for other diagnoses change after HAART.

E N D
Figure 2. Hospitalization Rates by Category Prior to and After HAART Abstract Background: Hospitalization rates for AIDS defining illnesses (ADI) decrease after HAART initiation. It is unclear how hospitalization rates for other diagnoses change after HAART. Methods: This is a prospective observational study of 2031 HIV-infected patients followed by the Johns Hopkins AIDS Service who first initiated HAART 1996 – 2005. Hospitalization rates and causes were examined before and after first HAART initiation. Modified Clinical Classification Software 2008 was used to assign the primary cause of each hospitalization to 1 of 18 diagnostic categories. Relative hospitalization rates were estimated using negative binomial regression. Results: The cohort was 34% female, 76% Black, 45% IDU, 27% MSM and had a median age of 39 years (IQR 34, 44). About half (54%) initiated HAART in 1996 to 1998. The median CD4 count and HIV-1 RNA level at HAART initiation were 152 cells/mm3 (37, 298) and 4.8 Log10 copies/mL (4.1, 5.3) respectively. Thirty-eight percent of subjects had > 1 hospitalization in the overall period from 180 days prior to HAART through 365 days afterward. Admissions due to any cause declined by 46 – 90 days after HAART (RR vs. 180 days prior, 0.76 [0.62, 0.93]). Non-ADI infections, ADI, psychiatric, GI and liver, endocrine / metabolic, renal, and cardiovascular were the seven most common diagnostic categories. Compared to the 180 days prior to HAART (Figure 2), statistically significant decreases in hospitalization rates were seen at 91 – 180 days after HAART for ADI (RR, 0.60 [0.42, 0.85]) and psychiatric illness (0.47 [0.26, 0.83]), and at 181 – 365 days for ADI (0.46 [0.33, 0.63]), psychiatric illness (0.60 [0.37, 0.98]), and non-ADI infections (0.72 [0.55, 0.94]). Virologic data to determine whether a subject had a significant response to HAART (> 1Log10 decrease in HIV-1 RNA within 6 months) were available for 1327 subjects. Among this group, virologic responders showed significant decreases in ADI and non-ADI infections after 90 days while non-responders did not. Conclusions: Hospitalization is common, and infections (both ADI and non-ADI) are the reasons for the majority of hospitalizations within the period surrounding HAART initiation. Providers should continue to be aware of the high risk of infectious illness through at least one year following HAART initiation, although decreases in risk of both infectious and psychiatric admissions may occur within 3 to 6 months. * * * * * * Indicates P<0.05 for the relative hospitalization rate compared to the rate 180 days prior to HAART initiation. O-219 CROI Montreal, QC February 8 – 11, 2009 Reasons for Hospitalizations that Occur after HAART InitiationStephen A Berry, Yukari C Manabe, Richard D Moore, Kelly A Gebo Johns Hopkins University School of Medicine, Baltimore, MD, USA Stephen A. Berry, M.D. 1830 E. Monument Street / Suite 452 Baltimore, MD 21287Phone: 410-502-8829 Fax: 410-537-7266Email: sberry8@jhmi.edu Figure 3.Hospitalization Rates by Virologic Response A.965 Virologic Responders * * * * * * Hospitalizations / 100 PY B.362 Non-Responders * * * * Interpretation: Hospitalizations for Non-AIDS defining infections, AIDS defining illnesses and psychiatric illnesses decreased statistically significantly within the year after HAART initiation, while hospitalizations for other illnesses did not. *Indicates P<0.05 for the relative hospitalization rate compared to the rate 180 days prior to HAART initiation. Hatched region indicates portion of ADI’s considered immune reconstitution inflammatory syndromes. Background HIV infection increases morbidity from opportunistic infections and other AIDS defining illnesses (ADI). While HAART may decrease risk for many illnesses over the long-term, disease rates following initiation are unknown. Our main objective was to measure hospitalization rates due to various causes over time in the year after HAART initiation. Interpretation: The decrease in infectious and psychiatric hospitalizations after HAART initiation occurs primarily among virologic responders. For virologic responders during days 1-45 after HAART initiation, immune reconstitution inflammatory syndromes account for >50% of hospitalizations due to AIDS defining illnesses and 13% of all hospitalizations. Conclusions Methods Figure 1. All-cause Hospitalization Rate Prior to and After HAART Initiation • All-cause hospitalization rate remains high (comparable to the pre-HAART rate) for the first 45 days after HAART initiation, then falls significantly between 45 and 90 days after initiation • In our cohort, Non-AIDS defining infections (Non-ADI Inf) and AIDS defining illnesses (ADI) are the top causes of hospitalizations prior to HAART initiation and throughout the following year • Hospitalization rates for both Non-ADI Inf and ADI remain high for 45 days then decrease; this pattern appears particularly true for virologic responders • Hospitalization rates for psychiatric illness also fall significantly after HAART initiation, but it may be that treatment of psychiatric illness leads to HAART initiation • Age, sex, race and IDU are associated with hospitalization risk for Non-ADI Inf and psychiatric illness whereas hospitalization risk for AIDS defining illnesses is most associated with CD4 count Hospitalizations prior to and after HAART initiation were examined for all HAART naïve patients in the Johns Hopkins HIV Clinical Cohort who initiated HAART 1996 – 2005. Professional abstractors assigned primary reasons for hospitalization by ICD-9 code. Modified Clinical Classifications Software (AHRQ, 2008) was used to classify reasons for hospitalization into 18 categories. Hospitalization rates were calculated per 100 person years (PY) for the periods: 180 days prior to HAART initiation and days 1–45, 46–90, 91-180, and 181–365 after HAART. Multivariate negative binomial regression with generalized estimating equations was used to estimate relative hospitalization rates and standard errors. For the 1327 persons with sufficient data, virologic response was defined as a decrease in HIV-1 RNA of >1 Log10 at 6 months after the HAART initiation. Among virologic responders, immune reconstitution inflammatory syndrome (IRIS) was identified by chart review. * * * Implications Clinically meaningful recovery of immune function becomes evident between 45 and 90 days after HAART initiation. Providers should maintain close clinical vigilance for opportunistic and non-opportunistic infections through at least 90 days even among virologic responders. * Indicates P<0.05 for the relative hospitalization rate compared to the rate 180 days prior to HAART initiation.



















