Download
1 / 1
10 likes | 121 Views
Development of Anxiety Among Depressed Veterans After Antidepressant Usage Zhiguo Li, Paul Pfeiffer, Katherine Hoggatt, Kara Zivin, Karen Downing and Marcia Valenstein SMITREC, Department of Veteran Affairs and University of Michigan, Ann Arbor, MI. Methods. Background.

E N D
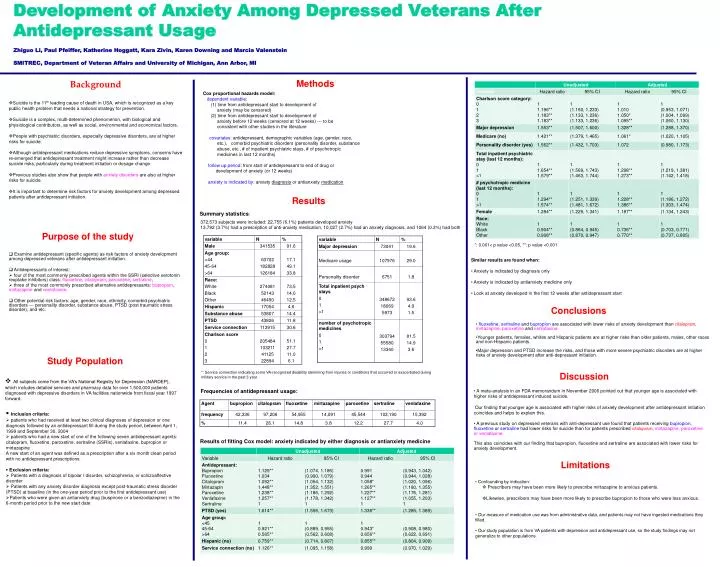
Development of Anxiety Among Depressed Veterans After Antidepressant Usage Zhiguo Li, Paul Pfeiffer, Katherine Hoggatt, Kara Zivin, Karen Downing and Marcia Valenstein SMITREC, Department of Veteran Affairs and University of Michigan, Ann Arbor, MI Methods Background Cox proportional hazards model: dependent variable: (1) time from antidepressant start to development of anxiety (may be censored) (2) time from antidepressant start to development of anxiety before 12 weeks (censored at 12 weeks) --- to be consistent with other studies in the literature covariates: antidepressant, demographic variables (age, gender, race, etc.), comorbid psychiatric disorders (personality disorder, substance abuse, etc., # of inpatient psychiatric stays, # of psychotropic medicines in last 12 months) follow up period: from start of antidepressant to end of drug or development of anxiety (or 12 weeks) anxiety is indicated by: anxiety diagnosis or antianxiety medication • Suicide is the 11th leading cause of death in USA, which is recognized as a key public health problem that needs a national strategy for prevention. • Suicide is a complex, multi-determined phenomenon, with biological and physiological contributors, as well as social, environmental and economical factors. • People with psychiatric disorders, especially depressive disorders, are at higher risks for suicide. • Although antidepressant medications reduce depressive symptoms, concerns have re-emerged that antidepressant treatment might increase rather than decrease suicide risks, particularly during treatment initiation or dosage change. • Previous studies also show that people with anxiety disorders are also at higher risks for suicide. • It is important to determine risk factors for anxiety development among depressed patients after antidepressant initiation. Results Summary statistics: 372,573 subjects were included: 22,755 (6.1%) patients developed anxiety 13,792 (3.7%) had a prescription of anti-anxiety medication, 10,027 (2.7%) had an anxiety diagnosis, and 1064 (0.3%) had both Purpose of the study *: 0.001< p value <0.05, **: p value <0.001 • Examine antidepressant (specific agents) as risk factors of anxiety development among depressed veterans after antidepressant initiation. • Antidepressants of interest: • four of the most commonly prescribed agents within the SSRI (selective serotonin reuptake inhibitors) class: fluoxetine, citalopram, paroxetine, sertraline, • three of the most commonly prescribed alternative antidepressants: bupropion, mirtazapine and venlafaxine. • Other potential risk factors: age, gender, race, ethnicity, comorbid psychiatric disorders --- personality disorder, substance abuse, PTSD (post traumatic stress disorder), and etc. • Similar results are found when: • Anxiety is indicated by diagnosis only • Anxiety is indicated by antianxiety medicine only • Look at anxiety developed in the first 12 weeks after antidepressant start Conclusions • fluoxetine, sertraline and bupropion are associated with lower risks of anxiety development than citalopram, mirtazapine,paroxetine and venlafaxine. • Younger patients, females, whites and Hispanic patients are at higher risks than older patients, males, other races and non-Hispanic patients. • Major depression and PTSD increase the risks, and those with more severe psychiatric disorders are at higher risks of anxiety development after anti-depressant initiation. Study Population *: Service connection indicating some VA-recognized disability stemming from injuries or conditions that occurred or exacerbated during military service in the past 3 year. Discussion • All subjects come from the VA’s National Registry for Depression (NARDEP), which includes detailed services and pharmacy data for over 1,500,000 patients diagnosed with depressive disorders in VA facilities nationwide from fiscal year 1997 forward. Frequencies of antidepressant usage: • A meta-analysis in an FDA memorandum in November 2006 pointed out that younger age is associated with higher risks of antidepressant induced suicide. • Our finding that younger age is associated with higher risks of anxiety development after antidepressant initiation coincides and helps to explain this. • A previous study on depressed veterans with anti-depressant use found that patients receiving bupropion, fluoxetine or sertraline had lower risks for suicide than for patients prescribed citalopram,mirtazapine, paroxetine or venlafaxine. • This also coincides with our finding that bupropion, fluoxetine and sertralineare associated with lower risks for anxiety development. • Inclusion criteria: • patients who had received at least two clinical diagnoses of depression or one diagnosis followed by an antidepressant fill during the study period, between April 1, 1999 and September 30, 2004 • patients who had a new start of one of the following seven antidepressant agents: citalopram, fluoxetine, paroxetine, sertraline (SSRIs), venlafaxine, bupropion or mirtazapine • A new start of an agent was defined as a prescription after a six month clean period with no antidepressant prescriptions. • Exclusion criteria: • Patients with a diagnosis of bipolar I disorder, schizophrenia, or schizoaffective disorder • Patients with any anxiety disorder diagnosis except post-traumatic stress disorder (PTSD) at baseline (in the one-year period prior to the first antidepressant use) • Patients who were given an antianxiety drug (buspirone or a benzodiazepine) in the 6-month period prior to the new start date Results of fitting Cox model: anxiety indicated by either diagnosis or antianxiety medicine Limitations • Confounding by indication: • Prescribers may have been more likely to prescribe mirtazapine to anxious patients. • Likewise, prescribers may have been more likely to prescribe bupropion to those who were less anxious. • Our measure of medication use was from administrative data, and patients may not have ingested medications they filled. • Our study population is from VA patients with depression and antidepressant use, so the study findings may not generalize to other populations.






















