Download
1 / 27
270 likes | 302 Views
This study focuses on estimating the population size of men who have sex with men (MSM) in Ghana using innovative methods such as service multipliers and unique object multipliers. By integrating bio-behavioral surveys with mapping techniques, it aims to provide accurate population estimates. Key assumptions and methodologies, including Successive Sampling-Population Size Estimate (SS-PSE), are explained in detail. Literature review, mapping methods, and validation steps are outlined to ensure the reliability and precision of the estimates.

E N D
Size Estimates of MSM: Ghana Men’s Study II MAPPING AND POPULATION SIZE ESTIMATION (MPSE) AND INTEGRATED BIO-BEHAVIORAL SURVEILLANCE SURVEY (IBBSS) AMONG MEN WHO HAVE SEX WITH MEN (MSM) IN GHANA (II ROUND OF NATIONAL SURVEY, 2017) NHARCON 2018
Population Size Estimates Methods • Service multiplier • Unique Object • Literature • SS-PSE(RDS-A) • Mapping
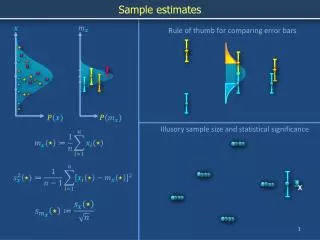
Service Multiplier • Two independent sources of data: • Source 1: HIV/AIDS services (e.g. HTS) • # of MSM accessing services[M] • Source 2: MSM survey (Indicates MSM at risk) • “In the past 6 months, have you received HTS?” • Obtain % or proportion of source 2 [P] • Needs to be representative of population • Population size (N) = M/P • Variance: V(N) = {Var(M)/[E(P)]2 }+{{[E(M)]2/[E(P)]4}*VAR(P)} • Standard error(se) = SQRT(V(N)) • 95% Confidence interval bound : point estimate +/-1.96(se)
Key assumptions: Service Multiplier • Two data sources are statistically independent • Survey population is representative of population of interest • Can result in over/under estimation • If Source 2 oversamples %MSM that get HTS the N will be lower than truth • If Source 1 HTS or service data quality: • lowreport of MSM may lead to underestimation • Double counting at HTS sites, repeat testing
Unique object Multiplier • Two independent and overlapping samples : • Source 1: “marked’ by distribution of unique objects( M) • Unique object- a locally made bracelet with a distinct pattern distributed to MSM in the geographic area of the full RDS survey • Source 2: representative sample of MSM from survey • “In the past 6 months, have you received a unique object (describe object)? “ • Obtain % or proportion of source 2 [P] • Population size (N) = M/P • Variance: V(N) = {Var(M)/[E(P)]2 }+{{[E(M)]2/[E(P)]4}*VAR(P)} • Standard error(se) = SQRT(V(N)) • 95% Confidence interval bound : point estimate +/-1.96(se)
Key assumptions: Unique Object Multiplier • Two data sources are statistically independent • Survey population is representative of population of interest Thus, • Unique object multipliers afford the greatest control and potentially most accurate estimates of size
Successive sampling -Population size estimate(SS-PSE) • SS-PSE uses a Bayesian framework, adopting prior knowledge or educated approximations of population size. • Assumes a posterior predictive distribution for population using data sources: • prior belief about population size. • Priors need not be precise, but provide a rough idea based on expert belief, estimates from other methods, literature review, etc. • Self-reported network size by participants’ • Order of sampling of participants indicated by the recruitment date.
Successive sampling -Population size estimate(SS-PSE) • Rather than use self-report network size, we used “impute visibility” to avoid errors including • coarsening (heaping or rounding) of responses • under or over reporting by participant. • Imputed visibility =f(self-reported network size) • Estimated from information collected during the RDS study. • Has a measurement error model to account for errors in self-reported network size.
Literature Review • Focused on a synthesis of local demographic data, local and international data on prevalence of key populations. • Review of published and grey literature • relevant data from similar cities and regions • to calculate benchmark estimates • to estimate proportion in the male population ( Example Ghana Men's study I provide estimates of % adult males in Population in surveyed and non surveyed sites
Mapping Method • Step 1: List of study regions /cities • Step 2: Visit regions /cities for ethnographic mapping of hotspots • Generate list of hotspots where MSM congregate or meet new sexual partners; estimate minimum and maximum MSM who frequent the hotspots; and a count of MSM found at hotspot • Participants • Secondary key informants (KIs) with information on locations or spots (‘‘hotspots’’). SKIs included people knowledgeable about their local area • from a variety of public places such as at taxi ranks, bus stops, fuel stations, shopping malls, streets, bars, and other workplaces. Also MSM peer educators or MSMs
..cont. Size estimation: Mapping Method • Step 2: Outputs • A comprehensive list of unique spots MSM • MSM typologies of the spots (for example, bar, street, massage parlour, among others) • operational dynamics of each spot (for example, peak and non-peak times) • Estimated minimum and maximum number of MSM at hotspots, and actual counts of MSM found at site
..cont. Mapping Method • Step 3: Validation of hotspots: re-visits of hotspots in step 2 to • Validate sites/spots from site owners or MSM on site; Ascertain the sites/spots were active or inactive (frequented by MSM) • obtain number of MSM (Minimum and Maximum); • Interview MSM on site to obtain data on frequency of visits (to adjust for double counting in size estimates ) • Approach • Use MSM peer educators through existing MSM programmes in each selected region or city, where they were available, to accompany the study team to the identified spots and • mobilise individual MSM for interviews on estimated MSM population at the spots. (Take all approach i.e. interview all MSM on site).
..cont. Size estimation: Mapping Method • Step 4: Size Estimation • Use Step 3 Data in generating population size estimates adjusted for duplication (using frequency of visits) • For spots not re-visited, use an average of the estimates from secondary key informants in Step 2
Consensus on estimates: Process • Round1: study team presented estimates and justifications for the estimates based on data generated from the various methods used • Round2 : participants/experts to discussed the initial estimates and also introduce new data outside the survey results, with appropriate justifications. • Round 3: established the best point estimate by region to be aggregated to the national size estimate. • Round 4: Participants agreed on a range (lower and upper bounds) that encompass the point estimate in the previous round.
Collaborating Institutions Research partners • Kwame Nkrumah University of Science and Technology (KNUST) • Human Sciences Research Council (HIV/AIDS, STIs and TB (HAST) research programme) • The Ghana AIDS Commission (GAC) • The Centers for Disease Control and Prevention (CDC) Coordination • GAC Funding • The Centers for Disease Control and Prevention (CDC)
Acknowledgements • Ghana Police Service • The Scientific Advisory Committee • We thank the study participants who consented and patiently went through the data collection process without whom we would not have had a GMS II. • The Maritime Life Precious Foundation (MARITIME), Ghana HIV/AIDS Network (GHANET), JSI, Centre for Popular Education and Human Rights, Ghana (CEPEHRG), MIHOSO, WAAF, WAPCAS, Kharis Foundation, Apt Sexual and Reproductive Health Foundation, 4H and the Community Development Alliance (CDA), Wa, for the immense support provided for community entry and mobilization. The support of the KomfoAnokye Teaching Hospital and Ghana Health Service Regional Hospital Laboratories is acknowledged.
Funders This research has been supported by PEPFAR through the U.S. Centers for Disease Control and Prevention (CDC) under the terms of Cooperative Agreement - Supporting the GAC for Coordination of the Multi-Sectoral Response to HIV/AIDS in Ghana under PEPFAR, GH000088/03- 05

![OVERVIEW OF THE HIV/AIDS SITUATION IN GHANA AND GHANA’S NATIONAL RESPONSE (GHANA MULTI-COUNTRY HIV/AIDS PROGRAM [MAP] PR](https://cdn0.slideserve.com/353831/slide1-dt.jpg)