Download
1 / 37
370 likes | 473 Views
Hematopoiesis is the process of blood cell formation involving stem cells, progenitors, and mature cells with specific functions. The system maintains homeostasis through self-renewal, differentiation, and cellular interactions in niches within the bone marrow. Understand the hematopoietic hierarchy, leukemic stem cells, myeloproliferative disorders, and key molecular events like JAK2V617F mutation.

E N D
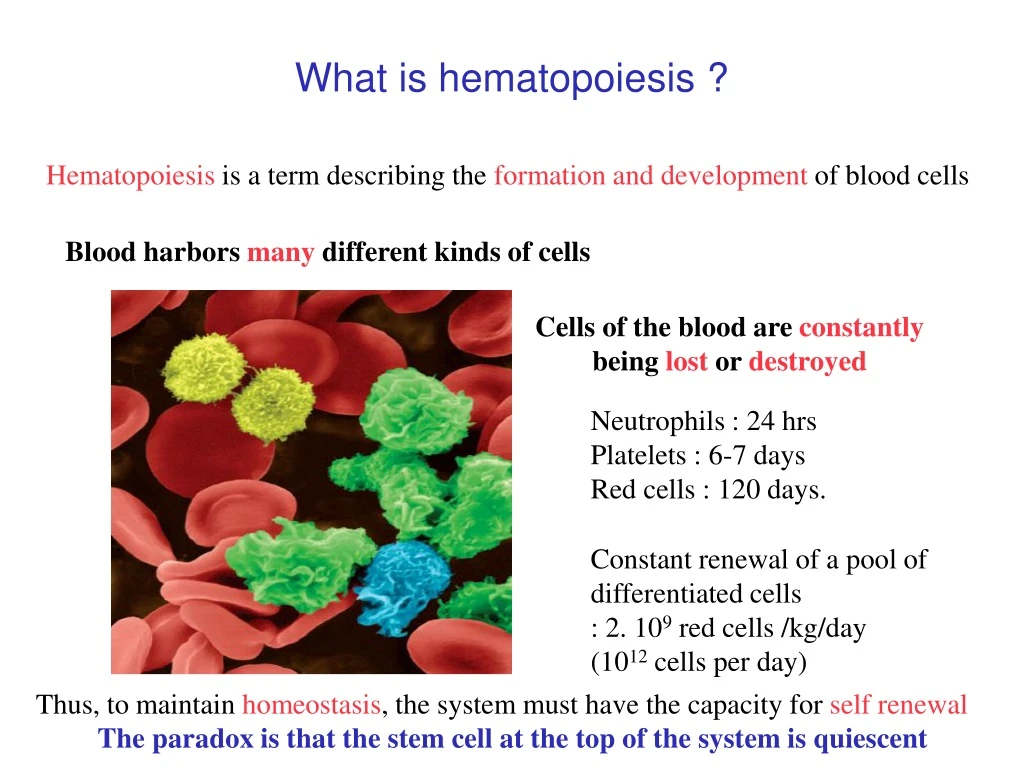
What is hematopoiesis ? Hematopoiesis is a term describing the formation and development of blood cells Blood harbors many different kinds of cells Cells of the blood are constantly being lost or destroyed Neutrophils : 24 hrs Platelets : 6-7 days Red cells : 120 days. Constant renewal of a pool of differentiated cells : 2. 109 red cells /kg/day (1012 cells per day) Thus, to maintain homeostasis, the system must have the capacity for self renewal The paradox is that the stem cell at the top of the system is quiescent
What is a stem cell Stem cell Self-renewal Differentiation Progenitors
Symmetric or asymmetric divisions Asymmetric division Stem cell Self-renewal Differentiation Symmetric divisions Progenitors Stem cell Stem cell Self-renewal Self-renewal Differentiation Progenitors Progenitors
Hematopoietic cells can be divided into three cellular compartments Hematopoietic stem cells (rare and undifferentiated) Hematopoietic progenitors Many intermediate states with varying degree of proliferation and differentiation Mature cells -with specific function (i.e. O2 transport) -represent most of the cells Sequential events leading to mature blood cells
Chimiokines (Il-8, SDF-1..) CAR cells Cytokines (Tpo, SCF, HGF, FGF4…) Osteoclasts Osteoblasts Proteases (MMP9, CTK…) Ang-1/Tie2 Wnt/β-caténin Jagged-1/Notch.. The bonemarrowhematopoietic niches Vascular niche Normoxia ESC CSM ECM (OPN) HSC Fibroblasts Hypoxia Ca++ Adipocytes Endosteal niche
HSC Morphogenes Cellular interactions BMP/TGFb Notch Wnt Shgh Chimiokines SDF1 Quiescence Self-renewal Differentiation Homing TPO SCF G-CSF Interferon Progenitors Cytokines Proliferation Differentiation Precursors Differentiation Cell functions
HSC 5x105-3x106 HSC Quiescence Self-renewal Differentiation Homing Average doubling time 45 days Asymmetric/symmetric division: 0.5-3 Extinction of stem cells (exhaustion, apoptosis) Progenitors Proliferation Differentiation 15 mitosis Precursors Differentiation Cell functions
Niche(Competition and clonal dominance) Symmetric division Asymmetric division Asymmetric division Symmetric division Symmetric division Asymmetric division Symmetric division Differentiation Clonal dominance induced by symetrical mitosis
The differentiation hierarchy of the hematopoietic system. Haeno H et al. PNAS 2009;106:16616-16621
CLP CMP Cancer stem cell/leukemic stem cellTumor is arranged as a hierarchy similar to normal hematopoietic tissue CD34+/ CD38- Quiescence Phenotype Niche dependency ? Leukemic stem cell HSC Leukemogenic events Bulk leukaemia cells Hematopoietic reconstitution Leukemia Block terminal differentiation Mature cells LSC LSC LSC HSC Progenitors Progenitors Progenitors Progenitors Precursors Precursors Precursors Precursors AML MDS MPD
The leukemic initiating genetic event can occur in an HSC or a progenitor by reprogrammation into a HSC Oncogenic event Oncogenic event Self-renewal
Classical MPDs CML Bcr-abl PDGFRa FGFR1 Kit WHO classification of MPDs Rare and unclassified MPDs Essential Thrombocythemia (ET) Polycythemia vera (PV) Myelofibrosis (PMF)
RBC RBC MPDs are clonal diseases involving HSC leading to increase blood cell production Normal hematopoiesis MPDs HSC PROGENITORS CFU-Eo CFU-MK BFU-E Pre-B Pre-T CFU-GM CFU-GM BFU-E CFU-Eo CFU-baso Pre-B CFU-MK CFU-baso Pre-T PRECURSORS CFU-E CFU-E NK B cell T cell PN Mono PEo PB B cell T cell NK PLT Mature cells Macrophage DC PMN Mono PMEo PLT PMB Macrophage DC
Clonal dominance of the MPD clones (log-log age incidence curve) RBC RBC 1/1x106 1x10-3 to 100% Up to 60 years HSC PROGENITORS CFU-Eo CFU-MK BFU-E Pre-B Pre-T CFU-GM CFU-GM BFU-E CFU-Eo CFU-baso Pre-B CFU-MK CFU-baso Pre-T PRECURSORS CFU-E CFU-E NK B cell T cell PN Mono PEo PB B cell T cell NK PLT Mature cells Macrophage DC PMN Mono PMEo PLT PMB Macrophage DC
JAK2 Exon 12 MPL W515 JAK2V617F 3%-5% 30% 95% 65% PV ET ? JAK2V617F K539L V617F JAK2V617F 50% 25% 45% 50% 5% MPL W515 atypical MPDs BCS PMF Molecular events and classical MPDs N-term C-term JH1 JH2 SH2 FERM domain Cytokine receptor Interacting domain Pseudokinase domain Kinase domain JAK2V617F Baxter, The Lancet 2005 James, Nature 2005 Kralovics, NEJM 2005 Levine, Cancer Cell 2005 JAK2 exon 12 Scott, NEJM 2007 MPL W515 Pickman, PLoS med 2006
A proposed structure of JAK2V617F Lee et al. Cancer 15, 1692, 2009
A G A N A C A A G A C A C A A G A A A C A C C C C C C T N A A G G G G The mutation is homozygous in 30% of the PV patients by duplication of the mutated allele N PV1 homozygous Granulocytes FISH JAK2: the two alleles are present PV2 heterozygous T cells This homozygosity correlates with 9pLOH (Kralovics et al 2005) and is related to a mitotic recombination
Allele ratio from blood leukocyte DNA in PV and ET patients N A G A A C A A A G A A C A PV Homozygous Heterozygous ? Homozygous ? ET
RBC RBC Clonal dominance in MPD clones ET PV CFU-Eo CFU-MK CFU-Eo CFU-MK BFU-E Pre-B Pre-T BFU-E Pre-B Pre-T CFU-GM CFU-GM CFU-baso CFU-baso CFU-E CFU-E NK NK B cell B cell T cell T cell PMN Mono PMN Mono PMEo PMEo PLT PLT PMB PMB Macrophage Macrophage DC DC
Is JAK2 signaling sufficient to induce a clonal dominance at the level of HSC ? (Requirement for other mutations such as TET2 ? ) ET PV (heterozygous profile) PV (homozygous profile) Clonal amplification PMF Normal marrow ET (heterozygous) PV heterozygous PV homozygous 1.0 Lympho- Myeloid progenitors CD34+/38- 0.8 0.6 Commited Progenitors (BFU-E, CFU-GM) Homo. JAK2V617F Size of the JAK2 V617F clone 0.4 Precursor cells Erythroblasts Granulocytes B cells, NK 0.2 Thrombocytosis Erythrocytosis Erythrocytosis Fibrosis 0.0 CD34+CD38- Erythroblasts Granulocytes CD34+CD38+
Chromosome 4 q24 MPD01 MPD04 MPD05 LOH 107.33 Mb SNP Array 106.11 Mb 106.35 Mb 325 Kb deletion MPD01 5' 3' TET2 MPD02 MPD05 Discovery of a cooperative genetic events Copy neutral LOH
CD19 CD56 TET2 CD15 CD15 TET2 loss of function:increase in HSC/progenitors or both ? Proliferative advantage Early onset of clonality Facilitates transformation by increasing cells targetted by oncogenic hits NOD-SCID HSC JAK2VF JAK2VF lympho-myeloid progenitor cell CD19 CD56 CFU-GM lymphoid progenitor cell MEP CD15 CD15 CFU-MK BFU-E JAK2VF CFU-G CFU-M CFU-E late onset of clonality Erythroblast NK Megakaryocyte B cell JAK2VF Monocytes T cell RBCs platelets Granulocytes
Modeling cancer disease A model of cancer initiation Haeno H et al. PNAS 2009;106:16616-16621
The probability of cancer initiation along the four evolutionary trajectories Haeno H et al. PNAS 2009;106:16616-16621
The dominant trajectory to MPN-initiating cells. Haeno H et al. PNAS 2009;106:16616-16621
Illustrative simulations showing age-specific incidence curves predicted from single mutation conferring an "exponential phenotype • Conclusions • Minimum 18 V617F HSC to get a phenotype • Symmetrical divisions (0.2-0.4/cell/year) • Loss of HSC through differentiation (0.8-0.95 the rate of symmetrical divisions) • 60%-99% of all clones are extinguished Vickers, M. A. Blood 2007;110:1675-1680
E14 Murine models to model the disease(KI Mice) TTC (F617) Promoter Expression E12 E13m CMVpromoter Cre embryonic / Ubiquitous VAVpromoter Cre embryonic / hematopoietic KI/Cre SCLpromoter CreERt Hematopoietic / inducible (tamoxifen)
Classical MPDs CML Bcr-abl PDGFRa FGFR1 Kit Modeling response to targeted therapiesThe model of CML WHO classification of MPDs Rare and unclassified MPDs Essential Thrombocythemia (ET) Polycythemia vera (PV) Myelofibrosis (PMF) CML is caused by a fusion protein BCR-ABL BCR-ABL can be targeted by Imatinib (a TK inhibitor) Clinical success but does not eradicate the disease Resistance to treatment can also appear
Response to therapy and modeling(Michor et al. Nature 2005) Two curves: The first corresponds to the killing of maturing cells The second to the effects on more primitive cells, Progenitor or stem cell ?
Exhaustion of HSC through proliferation(the exemple of interferon) Trump et al.
Polycythemia Vera and pegylated Interferon alpha (Kiladjian et al. Blood, 2008) Effect on a leukemic stem cell ?
RBC Minimum 18 V617F HSC to get a phenotype Drugs which would activate HSC (Interferon ?) 1x10-3 to 100% CFU-Eo CFU-MK BFU-E Pre-B Pre-T CFU-GM CFU-baso CFU-E NK B cell T cell Drugs which would kill specifically the proliferating mutated cells (specificic JAK2 inhibitor) PMN Mono PMEo PLT PMB Macrophage DC
Conclusions • Modeling of normal hematopoiesis may be a powerful tool to predict complex biologic processes that will be validated by experimental procedures • Modeling of malignant hematopoiesis may help to understand the clonal dominance and the cooperative effects of several genetic alterations • Modeling might be a powerful tool to prospectively in vivo monitor the response to a drug and a combination of drugs • MPD appear to be disorders whose pathogenesis and treatment might be greatly improved by such an approach
Acknowledgments • INSERM U1009 • Villejuif • Eric Solary • François Delhommeau • Nicole Casadevall • Stéphane Giraudier • Rodolphe Besancenot • Jean-Pierre Le Couédic • Isabelle Plo • Jean Luc Villeval Ludwig Institute for Cancer Research (Brussels) Stefan Constantinescu INSERM U985 Villejuif Olivier Bernard Véronique Della Valle Roland Berger




















