Download
1 / 34
340 likes | 565 Views
The effectiveness of cost-effectiveness of analysis: Stories of two practitioners. Elliot Marseille, MPP, DrPH Institute for Health Policy Studies University of California, San Francisco February 15 , 2007 DCEA. HIV in the Developing World. 38.6 million HIV+ worldwide in 2005 (UNAIDS,2006)

E N D
The effectiveness of cost-effectiveness of analysis: Stories of two practitioners Elliot Marseille, MPP, DrPHInstitute for Health Policy StudiesUniversity of California, San Francisco February 15, 2007 DCEA
HIV in the Developing World • 38.6 million HIV+ worldwide in 2005 (UNAIDS,2006) • 4.1 million newly infected • 2,8 million lost their lives • 25 million HIV+ in sub-Saharan Africa • In 1999, HIV caused 20.6% of deaths. • Life expectancy in the worst affected countries is down by 20 years. • The most productive members of the society are decimated, GDPs in decline (?) • Peril on the “frontier countries”: India (5.2 m), China (650K), Russia (940K)
HIV Prevention, Developing World • Prevention works: • Behavior change interventions in high risk groups, eg CSWs increase condom use 48% (5 published studies). • Voluntary counseling and testing effective with discordant couples: 60% higher condom use (2 published studies). • STI treatment highly effective especially early in epidemic, HIV incidence down by 37-62% (2 published studies) • Male circumcision high acceptability in many SSA countries; effectiveness of 50% - 60%. (2 trials plus ecological data) • Insufficient research on IDUs, youth, MSMs, HIV+, structural interventions. • Thus, failure of prevention funding, not prevention.
Mother-To-Child-Transmission (MTCT) in the US: 1985-1999 250 200 150 Number of Cases 100 What happened? Answer: ARVs 50 0 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 1985 Quarter-Year of Diagnosis Source: CDC 2000.
Economic Analysis of the HIVNET 012 Results – Implications for Policy Elliot Marseille, Dr.P.H., M.P.P - Health Strategies International James G. Kahn, M.D., M.P.H. - University of California, San Francisco Francis Mmiro, MBChB, FRCOG - Makerere University, Kampala Laura Guay, M.D. - Johns Hopkins University Philippa Musoke, MBChB - Makerere University, Kampala Mary Glenn Fowler, M.D. Centers for Disease Control and Prevention J. Brooks Jackson, M.D. - Johns Hopkins University
Research Questions • Is the HIVNET 012 regimen cost-effective in Sub-Saharan Africa? (Under what circumstances would it not be cost-effective?) • How does the cost-effectiveness of the HIVNET 012 nevirapine regimen compare with that of other ARV-based vertical transmission interventions? • What do these results suggest about program design and policy?
Analytic Approach - 1 • Standard cost-effectiveness analysis from perspective of public-sector health care payer. • Literature-based estimates of inputs. • Assessment of HIVNET 012 under two scenarios: • Targeted treatment (HIV counseling and testing) • Universal treatment (no HIV counseling and testing)
Analytic Approach - 2 • Extensive sensitivity and threshold analyses. • Conservative biases compared with other analyses: • Saved HIV/AIDS treatment costs are not • included as a program benefit. • Model assumes no adult-to-adult HIV prevention • benefit of counseling and testing.
Cost-Effectiveness of HIVNET 01220,000 mothers and 15% HIV prevalence
Threshold Analysis Input values needed for $50/DALY - (targeted)
Cost per DALY of HIVNET 012 as a function of HIV-1 seroprevalence
Findings • HIVNET 012 is likely to be highly cost-effective in sub-Saharan Africa. • It is more economical than other ARV interventions proven to be effective in developing countries. • Cost-effectiveness is maintained in low prevalence and in high cost settings. • Universal treatment (no VCT) is more economical than targeted treatment. This finding is sensitive to assumptions about the external benefits of VCT.
Implications for Policy - 1 • Assuming confirmation of HIVNET efficacy by additional trials, NVP should become front-line treatment in resource-poor countries. • Where prospects for establishing VCT are poor, universal provision should be considered on an interim basis.
Implications for Policy - 2 • Confirmation of NVP’s apparent benefit in reducing post-natal risk is an urgent research priority. (DONE!!) • Program planners should consider implementation in lower prevalence settings in addition to the extremely high prevalence settings usually targeted for MTCT prevention. (DONE!!)
Cost-effectiveness of a program of home-based ART delivery in rural UgandaElliot Marseille, DrPH, MPPJasme G, Kahn, MD, MPPChristian Pitter, MD, MPHRebecca Bunnell, MD, MPH William Epalatai, MD Emmanuel Jawe Willy Were, MD David Moore, MD, MPH Jonathan Mermin, MD, MPH
Setting • Rural Tororo District (Eastern Uganda) • CDC/TASO home-based care package for HIV-affected families • Hygiene and sanitation education • VCT for family, HIV risk reduction counseling • CTX prophylaxis, safe water vessel • Malaria bed nets, TB screening and treatment • Weekly diagnosis/treatment of diarrhea and malaria • ART for 1,045 clients • ART when CD4 <250 or WHO stage 3 or 4 • 1st line NNRTI regimen ($182 ppy); 2nd line PI-containing regimen ($1,080 ppy)
Methods • Cost and benefits based on empirical results from 2 years of ART • Projected future costs and benefits of treatment during 2 years • Incremental CE following basic home-based care package • Outcomes: • ART program costs net of reduced medical care costs • Benefits to ART recipients • Averted HIV infections
Inclusion of previously unquantified ART benefits • PMTCT • Secondary transmission reduction through behavior change and lower viral loads • Reduced mortality in uninfected children of ART recipients
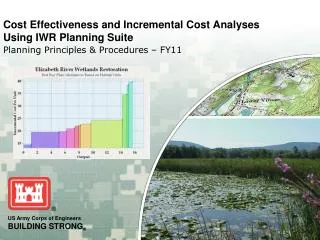
Comparison with two other ART CEAs • Cost saving for patients with AIDS; $675 per LY gained for non-AIDS patients. (Badri et al, PLoS Medicine, 2006) • $1,631 per QALY gained (Cleary et al, 2004) Thus, Tororo study at $615 per DALY averted incremental to CTX = relatively favorable CE.
Sources of DALYs averted due to ART Prevention components account for ~35%
Conclusions • Rural home-based ART can be cost-effective. • ART cost-effectiveness is more attractive when accounting for prevention and other benefits, but still in the same range. • ART is not cost-effective as prevention.
Areas for potential study refinement • 2 years of data only • Effect of including additional years in CE: Negative • Adverse drug reactions • Effect of including in CE: Negative • Greater longevity (opportunity for transmission) • Effect of including in CE: Negative
Unquantified ‘Macro’ effects of ART • scale-up
Unquantified ‘Macro’ effects of ART scale-up - # 1 Community ARV resistance Effect on CE: Negative but possibly small Adherence high in developing countries (very high in Tororo)
Unquantified ‘Macro’ effects of ART scale-up - # 2 Shift of resources away from other health activities (?) Effect on CE: Negative and potentially important “… in Africa many grass roots organizations and non-governmental organizations for people living with HIV, which were traditionally involved in community mobilization and prevention, have shifted their focus to treatment support activities.” Van Damme, W. et al. AIDS 2006 The real challenges for scaling up ART in sub-Saharan Africa. Editorial Review. Thailand reduced spending on prevention by 75% in 1997 – 2003. Prevention accounted for 8% of all HIV spending in 2003. (UNDP, Thailand’s response to HIV/AIDS,2004)
Unquantified ‘Macro’ effects of ART scale-up – # 3 Scale effects Effect on CE: Probably net positive Community ‘risk compensation’ Effect on CE: Probably net negative
Cost-effectiveness is only one input of the policy process Others include: • Equity (justice) • Public health impact (program scale) • Feasibility (administrative, financial) • Politics (art of the possible)
Politics Analysis Political process determines policy not economic appraisal. But analysis can help determine what is on the political agenda.