Download
1 / 19
190 likes | 289 Views
Central Okanagan PALLIATIVE MED REC Home and Community Care. Background. Palliative Clients who are admitted to Hospice for Pain and Symptom Management (PSM).

E N D
Central Okanagan PALLIATIVE MED REC Home and Community Care Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Background • Palliative Clients who are admitted to Hospice for Pain and Symptom Management (PSM). • Patient risk = loss of pain control; anxiety around uncertainties in medication also causes increased pain levels • Hospice temporarily located within a Residential setting until stand- alone site is ready Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Background • Multidiscliplinary team – Community, Acute, Residential, and Cancer Centre • Goals are to: • Expedite transitions • Prevent Adverse Drug Events in transitions • Project started just prior to Learning Session 1 in Saskatoon • Project charter draft written prior to LS1 Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim #1 4 Aim Statements: • Create Best Possible Medication History (BPMH) for 95% of the identified Palliative group within 24 hrs of admission to Hospice, and identify the discrepancies. The target date is Apr. 30, 2008. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim #2 & #3 • Reconcile 100% of the identified discrepancies within 48 hrs of admission, by Apr. 30, 2008. • Create a Best Possible Medication Discharge Plan (BPMDP) for 95% of patients transitioning back to the Community, by Apr. 30, 2008. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Aim #4 • Reduce Edmonton Symptom Assessment System (ESAS) score for symptom management by 50% by Apr. 30, 2008. (ESAS scores nine symptoms – pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, wellbeing and shortness of breath - on a scale from 0 to 10, with 10 being the worst possible symptom score. A reduced score would show improvements in symptom management.) Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Team Members • Community Care Manager • Director, Residential Services • Clinical Practice Consultant, Home Care Nursing (HCN) • Clinical Resource RN’s (Acute, Hospice & HCN Palliative Care) • Cancer Centre RN • Pharmacists (Clinical & Community) • Family Practitioner • Quality Improvement (SHN) Rep Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Changes Tested Who is completing BPMH? Clinical resource nurse. • Tested may different forms, only to fine tune an already existing form created in our acute care setting. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Changes Tested • Tested best timing to complete BPMH to have an accurate completed Med Rec done. • BPMH within 48hrs of admission with a goal of 1 week to Med Rec by Physician. b) BPMH within 24hrs of admission with a goal of 1 week to Med Rec by Physician c) BPMH on admission with Med Rec within 24 hrs of admission. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results • Forms tested….. Ours fine tuned. Tested 6 forms. • Timing….. We found doing a BPMH on admission to unit resulted in physicians completing the reconciliation soon after admit, with physician cooperation completing the Med Rec with appropriate, accurate orders. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results • Clients are often admitted to unit when CRN is not available. The target group is not always having a Med Rec completed with in the target timeframe. • Process Map prior to Med Rec created. • Process map and limited data follows… Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
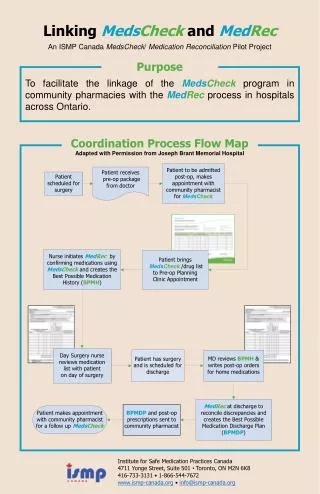
Process Map Prior to Med Rec Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results June: incomplete data ; CRN away.BPMH complete = 1 July (after July 23) P&SM admits = ? BPMH complete = 0 August P&SM admits = ? BPMH complete = 4 September (to date) P&SM admits = ? BPMH complete = 2 Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Results Run Charts of your Key Measures • Insert your run charts here (More than one slide may be necessary) • Annotate your run charts with specific changes you’ve tested Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Example of Annotated Graph:Improved Access (delete this slide before saving) Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Keys to Success and Lessons Learned • We need to expand our team educate and include bedside nurses in the process with 1 or 2 to take on the role of champions when the CRN is not available to complete the BPMH. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Keys to Success and Lessons Learned • One person completing the BPMH is too heavy a load! • Persistence! We need to persevere with follow up to get the physicians understand the importance of completing the med rec. • Process takes longer than anticipated; but well-designed form shortens and smoothes out the process. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Next Steps • We are aiming for hospice staff buy in and participation in creating a BPMH for each pain and symptom management client admitted to the hospice unit. • Adopt a BPMH/Med Rec form that includes our measurement components. • Include ESAS (Edmonton Symptom Assessment Scale) measurements on admit and discharge for all the Med Rec clients. Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative
Contact Information • Dianne Stockwell (Clinical Resource Nurse) dianne.stockwell@interiorhealth.ca (250) 862-4109 • Faye Burch (Director, Residential Services) faye.burch@interiorhealth.ca (250) 870-5784 • Holly Morgan (Clinical QI Coordinator) holly.morgan@interiorhealth.ca (250) 862-4300 Ext 7210 Coming Full Circle: AMI & Med Rec Across the Continuum Western Node Collaborative