Download
1 / 15

E N D
Risk factors for Incident Trichomonas vaginalis among Women Recruited in RESPECT-2, an HIV Prevention TrialD Helms 1, D Mosure 1, T Peterman 1, C Metcalf 1,2, J Douglas, Jr.1,3, CK Malotte 4, S Paul 51 Centers for Disease Control and Prevention, Division of STD Prevention, Atlanta, GA 2 Aurum Institute for Health Research, Johannesburg, South Africa 3 Denver Health, Denver Colorado4 California State University, Long Beach, CA 5 New Jersey Department of Health and Senior Services, Trenton, NJ
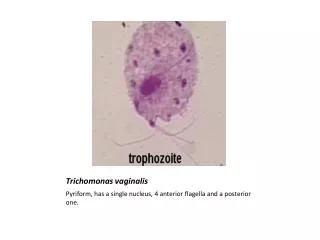
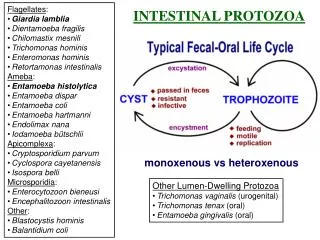
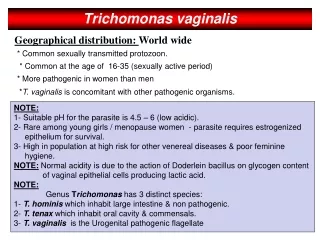
Trichomonas vaginalis • Most common non-viral STD • 5 million new infections occurring in the US annually • 50% of infected females are asymptomatic • Associated with adverse birth outcomes: premature rupture of the membranes, pre-term delivery, and low birth weight • May increase susceptibility to, or transmissibility of, HIV • Treatment cures 90-95% of infections
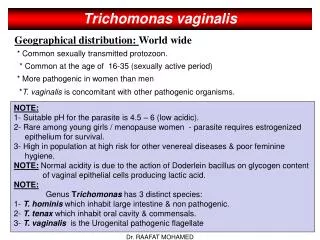
Epidemiology of T. vaginalis • Prevalence typically ranges from 5-10% in women in the general population • Risk factors for prevalent trichomonas infection include: black race, history of previous STDs, sex workers, pregnancy, multiple partners, and drug use • One incidence study has been conducted* One county in China In women aged >25 years Incidence rate of 1.1 per 100 person-years *Sex Trans Dis 1996; 415-424.
Objective • To determine risk factors associated with prevalent and incident trichomonas infection
Methods • Data from an HIV-prevention counseling trial (RESPECT-2) • 3 STD clinics in Long Beach, CA; Denver, CO; and Newark, NJ; 1999-2001 • 1507 women aged 15-39 years • Screened for STDs (chlamydia, gonorrhea, trichomonas) at baseline, 3, 6, 9, and 12 months • Wet mount or culture was used to test for trichomonas infection
Analysis • Prevalent trichomonas infection • Stratified by demographic, behavioral, and clinical risk factors • Incident trichomonas infection • New Infection – • Negative test at baseline and positive test at follow-up or • Positive test at least 14 days after treatment • for a baseline infection • Stratified by demographic, behavioral, and clinical risk factors • Logistic regression was used to identify risk factors
Results 1507 women 1462 tested by wet mount or culture for T. vaginalis at baseline 1269 tested at least once in follow-up* 190 (13%) prevalent infections 168 (13%) incident infections *Average duration of follow-up = 364 days
New and Repeat Infections 1462 women Baseline 190 positive 1272 negative 62 repeat 108 new infections Follow-up Total Incident 168 total incident infections Asymptomatic 121 (72%) asymptomatic
Risk Factors for Prevalent and Incident Trichomonas Infection CharacteristicsPrevalent % (N)Incident % (N) Age (years) 15-19 7.2 (359) 10.6 (303) 20-24 13.9 (461) 11.1 (395) 25-29 13.3 (278) 11.3 (240) 30-34 6.9 (195) 16.9 (178) 35-39 17.8 (169) 22.9 (153) Race/Ethnicity White 5.9 (307) 4.9 (268) Hispanic 6.5 (260) 6.1 (228) Other 7.6 (170) 6.5 (154) Black 19.6 (725) 21.2 (619) Education < 12 years 16.2 (413) 17.6 (358) > 12 years 14.4 (992) 14.6 (856)
Risk Factors for Prevalent and Incident Trichomonas Infection CharacteristicsPrevalent % (N)Incident % (N) Partners Past 3 Months 0 ▬ 10.7 (224) 1 11.4 (747) 10.1 (751) 2 13.7 (387) 18.9 (180) >3 15.9 (320) 23.6 (89) Sex for drugs/money1 Yes 26.3 (95) 40.0 (30) No 12.1 (1359) 12.0 (990) Symptoms of Trich2 Yes 7.5 (752) 22.1 (213) No 5.5 (710) 11.5 (1056) Chlamydia2 Yes 21.5 (181) 36.8 (38) No 11.8 (1268) 12.3 (1169) Gonorrhea2 Yes 22.7 (97) 38.5 (26) No 12.3 (1355) 12.4 (1187) 1Ever exchanged sex for money or drugs 2At time of trichomonas infection or at the last study interval
Multivariate analysis Trichomonas Infection PrevalentIncident Risk FactorsAOR95% C.I.AOR95% C.I. Age (years) 15-19 1.0 - 1.0 - 20-24 2.2 (1.3-3.6) 1.1 (0.6-2.0) 25-29 2.3 (1.3-4.0) 1.3 (0.7-2.7) 30-34 2.4 (1.3-4.4) 1.8 (0.9-3.6) 35-39 2.6 (1.4-4.7) 2.9 (1.4-6.0) Black 3.0 (2.0-4.5) 3.9 (2.3-6.7) >12 years of education 1.6 (1.1-2.3) 1.9 (1.2-3.0) Sex for drugs/money1 2.0 (1.1-3.3) 2.6 (1.1-6.2) Partners past 3 months ▬ 2.4 (1.5-3.7) Symptoms2▬ 2.4 (1.9-8.9) Chlamydia2 3.7 (1.6-8.3) 4.1 (1.6-8.3) 1Ever exchanged sex for money or drugs 2At time of incident trichomonas infection or at the last study interval
Limitations • Results reflect women in STD clinics • RESPECT-2 was not designed to evaluate risk factors associated with trichomonas infection • Possible misclassification of incident infections • Due to low sensitivity of wet mount or culture • Due to drug resistant infection
Conclusions (1) • Trichomonas infection is a common infection • 13% of women had a prevalent infection • 13% of women had an incident infection • High percentage of asymptomatic incident infection • Similar risk factors for prevalent and incident infection: • Older age (>35 years), Black race, concurrent chlamydial infection, and sex for drugs/money • Multiple partners and symptoms of trichomonas are risk factors for incident infection
Conclusions (2) • Future studies might consider additional information regarding, contraceptive method and whether the women douched • Unlike other STDs (gonorrhea and chlamydia), T. vaginalis was associated with older age in women • Further investigation should be done to determine if routine screening in STD clinics would be beneficial The findings and conclusions in this presentation are those of the author(s) and do not necessarily represent the views of the Centers for Disease Control and Prevention