Download
1 / 26
450 likes | 1.87k Views
Flagellates : Giardia lamblia Dientamoeba fragilis Chilomastix mesnili Trichomonas hominis Enteromonas hominis Retortamonas intestinalis Ameba : Entamoeba histolytica Entamoeba dispar Entamoeba coli Entamoeba hartmanni Endolimax nana Iodamoeba bütschlii Apicomplexa :

E N D
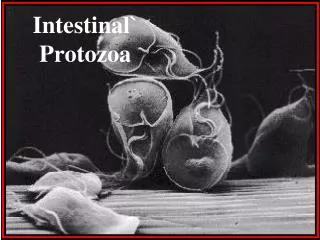
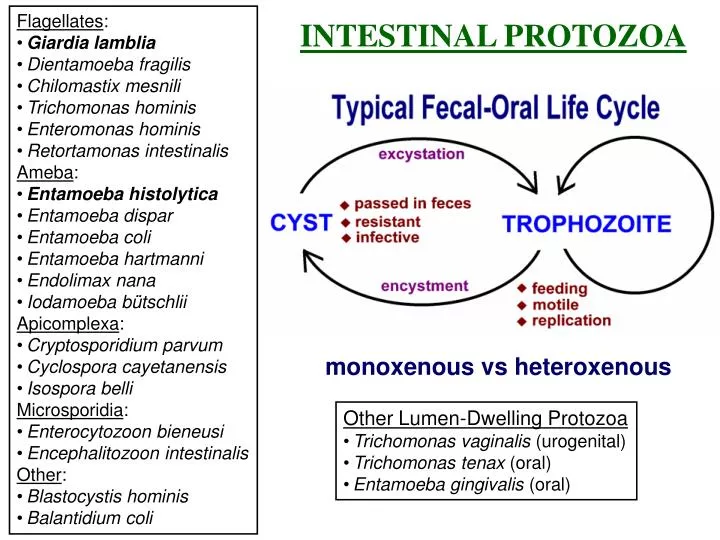
Flagellates: • Giardia lamblia • Dientamoeba fragilis • Chilomastix mesnili • Trichomonas hominis • Enteromonas hominis • Retortamonas intestinalis • Ameba: • Entamoeba histolytica • Entamoeba dispar • Entamoeba coli • Entamoeba hartmanni • Endolimax nana • Iodamoeba bütschlii • Apicomplexa: • Cryptosporidium parvum • Cyclospora cayetanensis • Isospora belli • Microsporidia: • Enterocytozoon bieneusi • Encephalitozoon intestinalis • Other: • Blastocystis hominis • Balantidium coli INTESTINAL PROTOZOA monoxenous vs heteroxenous • Other Lumen-Dwelling Protozoa • Trichomonas vaginalis (urogenital) • Trichomonas tenax (oral) • Entamoeba gingivalis (oral)
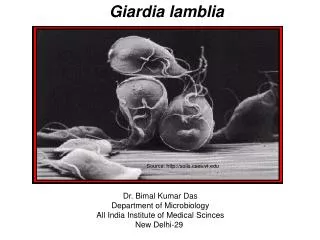
Giardia lamblia • worldwide distribution • higher prevalence in tropical or developing countries (20%) • 1-6% in temperate countries • most common protozoa in stools • ~200 million cases/yr • giardiasis • often asymptomatic • acute or chronic diarrhea Historical Notes 1681 van Leeuwenhoek observed 1859 Lambl documented 1920’s clinical symptoms, but controversial 1954 Rendtorff fulfilled Koch’s postulate • Taxonomy • one human species, aka: • G. duodenalis • G. intestinalis • morphologically similar forms in other mammals
Is giardiasis a zoonosis? • no definitive documentation • transmission between humans and dogs rare (J.Parasit. 83:44, 1997) • person-to-person trans-mission is most prevalent Fecal-Oral Transmission Factors • poor personal hygiene • children (eg, day care centers) • food handlers • developing countries • poor sanitation • endemic • travelers diarrhea • water-borne epidemics • male homosexuality • oral-anal contact • zoonosis? • Entamoeba =no • Cryptosporidium =yes • Giardia =controversial
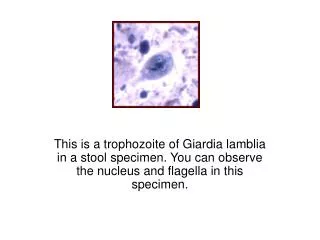
Giardia Life Cycle TROPHOZOITE CYST Infective stage passed in feces Replicative stage inhabiting sm. intestine
In Vitro Culture of Giardia • Excystation • brief exposure to acidic pH (~2) • flagellar activity within 5-10 min after return to neutral pH • breakdown of cyst wall (proteases) • trophozoite emerges from cyst • cytokinesis within 30 min • Encystation • exposure to pH 7, no bile • exposure to pH 7.8, high bile • cyst wall secretion (appearance of vesicles) • loss of disk and flagella • nuclear division
microtubules + microribbons lateral crest Adhesive Disk Components • microtubules • tubulin • microribbons • giardins • lateral crest • actin-myosin • Attachment Mechanisms? • contractile ring • hydrodynamic force • receptor mediated
Clinical Features and Symptoms • Subacute/Chronic • recurrent diarrheal episodes • cramps uncommon • sulfuric belching, ano-rexia, nausea frequent • can lead to weight loss and failure to thrive • Range of Outcomes • asymptomatic/latent • acute short-lasting diarrhea • chronic/nutritional disorders • Acute Symptoms • 1-2 week incubation • sudden explosive, watery diarrhea • bulky, frothy, greasy, foul-smelling stools • no blood or mucus • upper gastro-intestinal uneasiness, bloating, flatulence, belching, cramps, nausea, vomiting, anorexia • usually clears spontaneously (undiagnosed), but can persist or become chronic
Pathogenesis • epithelial damage • villus blunting • crypt cell hypertrophy • cellular infiltration • malabsorption • enzyme deficiencies • lactase (lactose intolerance) • Possible Mechanisms • mechanical irritation • obstruction of absorption
Diagnosis • suspect: acute or chronic symptoms • confirmed: detection of parasite in feces or duodenal aspirate or biopsy • parasite easy to identify • parasite can be difficult to detect • inconsistent excretion in feces • patchy loci of infection • Parasite Detection • Stools • 3 non-consecutive days • wet mounts or stained • IFA, copro-antigens • Aspirate or Biopsy • Enterotest (or string test)
Control • avoid fecal-oral transmission • improve personal hygiene • especially institutions • treat asymptomatic carriers • eg, family members • health education • hand-washing • sanitation • food handling • protect water supply • treat water if questionable • boiling • iodine • not chlorine Treatment • Drug of Choice • metronidazole (Flagyl) • 750 mg/tid/5d • >90% cure rate • Alternatives • tinidazole (single dose) • paromomycin (pregnancy) • quinicrine • furazolidone Prognosis is good with no sequelae
TRICHOMONADS • 3-5 anterior flagella • one undulating membrane • axostyle • hydrogensome (EM)
Trichomonas vaginalis • trophozoite stage transmitted during sexual intercourse • non-sexual contact possible • common STD • co-infection w/other STDs • more prevalent in at risk groups • associated with epithelium of uro-genital tract • females: vagina • males: urethra, prostate, epididymis • both sexes equally susceptible • symptoms more common in females sexual intercourse
Trichomoniasis In females: • ranges from asymptomatic, to mild or moderate irritation, to extreme vaginitis • 50-75% abnormal discharge (frothy, yellowish or greenish) • 25-50% pruritis • 50% painful coitus • onset or exacerbation often associated with menstruation or pregnancy • vaginal erythema, ‘strawberry cervix’ (~2%) In males: • 50-90% are asymptomatic • mild dysuria or pruritus • minor urethral discharge
DIAGNOSIS • demonstration of parasite • direct observation or in vitro culture • vaginal discharge • urine sediment • prostatic secretion • TREATMENT • metronidazole (Flagyl) • 250 mg (3/d) for 5-7 days • single 2 g dose • simultaneous treatment of partner! (85-90% cure rate) • PREVENTION • limit # of sexual partners • condoms
Key Features of Cysts • oval shape • 11-14 x 6-10 m • distinct cell wall set apart from cytoplasm • 4 nuclei at anterior end • large karyosome, no peripheral chromatin • fibrils (axonemes) evident • median bodies
Key Features of Trophozoites • pear shape • 12-15 x 5-10 x 2-4 m • 2 nuclei • large karyosome, no peripheral chromatin • fibrils (axonemes) evident • bilateral symmetry • pair of median bodies • adhesive disk (not always evident) • 4 pair flagella • motility likened to falling leaf
Other Flagellates Found in Human Feces • Dientamoeba fragilis • no flagella (discuss with amebas) • Pentatrichomonas hominis • formerly called Trichomonas hominis • Chilomastix mesnili • Enteromonas hominis • Retortamonas intestinalis
Non-Pathogenic Intestinal Flagellates Trichomonas hominis • 7-15 mm trophozoite • no cyst • single nucleus • axostyle • 4 free flagella + undulating membrane • costa
Non-Pathogenic Intestinal Flagellates Chilomastix mesnili • 10-20 mm trophozoite • 6-20 mm cyst • single nucleus • 4 flagella • cytostome
T. hominis Chilomastix mesnili